Knee injuries in combat sports
Why does my knee hurt when I shoot?
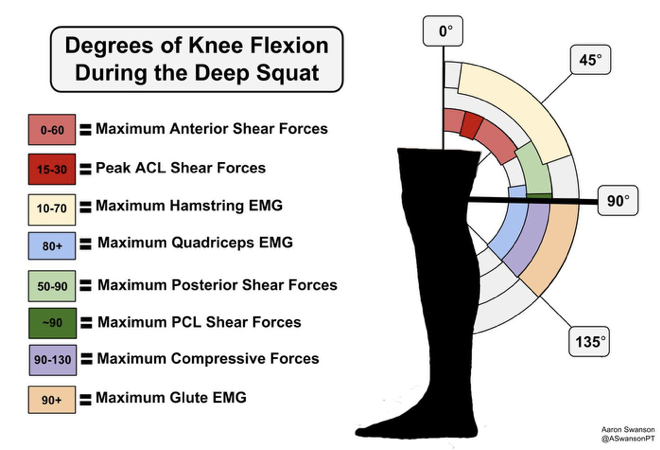
Anatomy: The knee is a relatively unstable joint because of the lack of bony congruency, or the amount of bony contact between the two joints. Ligaments, capsules & muscles work in concert to prevent excessive movement. There are four bones that make up the knee: the patella (knee cap), femur, tibia and fibula. The large femur forms two oval shaped balls which rests on the flat surface of the tibia. The knee cap provides a site of attachment for the large quadriceps muscle group, situated within a “groove” on the front part of the femur. The fibula (bone on the side of the leg) also provides an anchor site for a handful of muscles. The meniscus, ligaments and joint capsule all provide stability to the knee. Depending on the angle of the knee, different parts of the ligaments are tight and limit movement in specific directions (imagine clasping your hands together to prevent your opponent from ripping an arm bar). If the structure (meniscus, ligament) is under a load it cannot handle, the tissue will tear. Take a look at the infograph. It demonstrates the angle of knee flexion at which various parts of the leg muscles are either active or the ligaments are checking movement. When the knee is in the early phase of a squat, the femur will slide forward, the ACL and hamstrings will check the movement. Squat a little further (about 90 degrees, or thigh parallel to the ground) and the PCL and quadriceps muscle group will check movement. Squatting lower than thigh parallel to the ground will activate the glutes while the knee comes under the greatest amount of compressive force. Symptoms of pain or instability in various degrees of knee flexion can help determine which structures are implicated in an injury.
Ligaments and menisci have a limited capacity to heal. The portion of a ligament that is torn will remain that way unless unless you undergo surgery. Without surgery, the remaining part of the ligament does have some capacity to adapt and retain strength. Specific exercises can improve muscle strength to make up for a lack of ligamentous stability.
Injury: Oftentimes there is more than one part of the knee that is damaged. The “Terrible Triad” includes an anterior cruciate ligament (ACL), medial collateral ligament (MCL) and medial meniscus tear. This can significantly complicate surgery, rehabilitation and return to sport as less than 50% of all athletes undergoing knee surgery will not return to sport (for various reasons). Less than half of the athletes that do return to sport, do so at their pre-injury level of skill. That means that more than 50% of those returning to sport post-op will have a clinically weaker knee.
Connor McGregor is a phenomenal example because his knee injury (the dreaded “Terrible Triad”), subsequent surgery and rehabilitation was a resounding success. Athletes with an unstable knee due to a ligamentous tear will require surgery because they are much more likely to develop a meniscus tear within the following year.
Prevention Tips: Because of the inherently unstable nature of the knee, a well designed strength and conditioning program is essential if you want to avoid surgery, the harmful side effects of medicine and time off from competition or training. The section on medical exercise therapy (MET) and sport specific strength & conditioning provide a sound approach to implementing an effective and efficient injury prevention program. There should be a healthy mix of calisthenics-based mobility exercises, plyometrics and heavy resistance for improving local muscle strength.