Bacterial infections are often accompanied by a fever. So if you’ve been feverish for a month, have back pain and haven’t seen a doctor about that…
Go see one now!
Cauda equina syndrome is a life-threatening condition. If you show these signs and symptoms you should seek immediate medical attention.
NOTE TO THE READER: THIS BLOG POST DOES NOT OFFER ANY MEDICAL ADVICE.
IT IS FOR INFORMATIONAL PURPOSES ONLY.
YOUR SPECIFIC CASE NEEDS TO BE DISCUSSED WITH A QUALIFIED HEALTH CARE PROFESSIONAL.
If you have been treated by a chiropractor, massage therapist, physical therapist, have been exercising & following their advice AND you have not significantly improved for the past month, then it might be a good idea to consider seeking additional imaging or someone else to help.
For example, you’ve been up and down with the recovery but nothing seems to quite “stick” to improve how you feel.
Are you interested in learning more about MRIs and low back pain?
And maybe finding a solution to your back pain so you can enjoy beautiful Miami?
I want to share a story about two gentlemen:
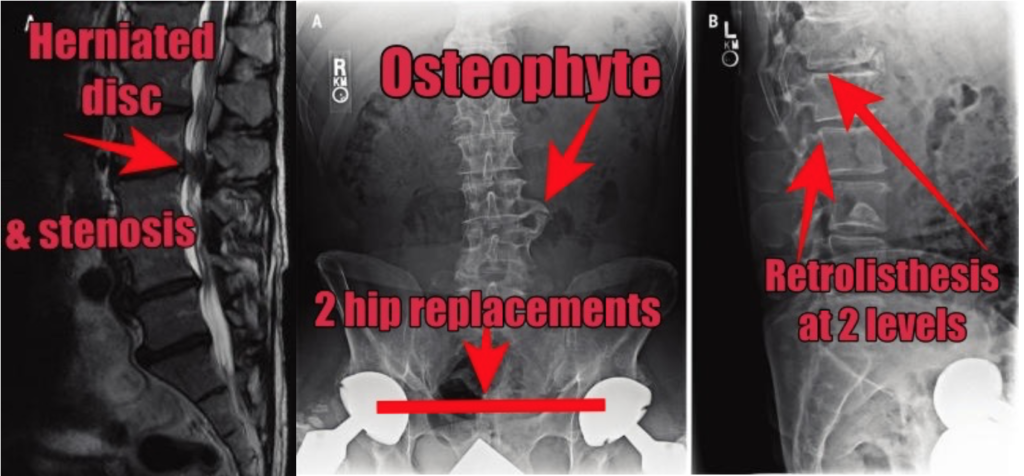
The first patient: a 62 year old with two hip replacements, significant lumbar degenerative disc changes at multiple levels, osteophyte formation, and a retrolisthesis of L1-2 and L2-3.
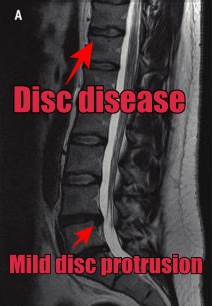
The second patient: a 32 year old mechanic with a history of chronic low back pain, took off of work on disability with an MRI that was “relatively unremarkable” with some degenerative disc disease of L4-5 and L5-S1 and mild disc protrusion at L4-5.
No nerve impingement. No hip replacement surgery. No additional bony outgrowth.
Who would you think had more pain, the first or second man?
Mr. 62-year-old had one single episode of back pain 8 years after his bilateral hip replacement-
…after canoeing and hiking for 2 WEEKS STRAIGHT!!
And he “WORKED THROUGH” the pain with stretching and ibuprofen while on his backpacking trip.
When he returned home, he had 9 sessions of physical therapy and then went on to backpack for another 2 weeks in the United States Continental Divide and had “0” back pain.
Superhuman?
Probably not.
Despite the growing field of research in injury assessment and risk management, there are quite a few unanswered questions. Standardization of measurements, sport-specific assessments, and more robust association in findings would help clear up many of these questions.
Practical application and programming for athletes and careers that require high fitness levels should also be discussed within the research community. Perhaps guidelines may help coaches develop pre-season injury assessments and provide strength and conditioning programs that are athlete-specific, essentially reducing the number of athletes sitting on the sidelines due to injury.
If you are an athlete or coach in Miami, FL and find this topic interesting, or want more information, reach out to our office for assistance.
Bacterial infections are often accompanied by a fever. So if you’ve been feverish for a month, have back pain and haven’t seen a doctor about that…
Go see one now!
Cauda equina syndrome is a life-threatening condition. If you show these signs and symptoms you should seek immediate medical attention.
NOTE TO THE READER: THIS BLOG POST DOES NOT OFFER ANY MEDICAL ADVICE.
IT IS FOR INFORMATIONAL PURPOSES ONLY.
YOUR SPECIFIC CASE NEEDS TO BE DISCUSSED WITH A QUALIFIED HEALTH CARE PROFESSIONAL.
If you have been treated by a chiropractor, massage therapist, physical therapist, have been exercising & following their advice AND you have not significantly improved for the past month, then it might be a good idea to consider seeking additional imaging or someone else to help.
For example, you’ve been up and down with the recovery but nothing seems to quite “stick” to improve how you feel.
Are you interested in learning more about MRIs and low back pain?
And maybe finding a solution to your back pain so you can enjoy beautiful Miami?
I want to share a story about two gentlemen:
The first patient: a 62 year old with two hip replacements, significant lumbar degenerative disc changes at multiple levels, osteophyte formation, and a retrolisthesis of L1-2 and L2-3.
The second patient: a 32 year old mechanic with a history of chronic low back pain, took off of work on disability with an MRI that was “relatively unremarkable” with some degenerative disc disease of L4-5 and L5-S1 and mild disc protrusion at L4-5.
No nerve impingement. No hip replacement surgery. No additional bony outgrowth.
Who would you think had more pain, the first or second man?
Mr. 62-year-old had one single episode of back pain 8 years after his bilateral hip replacement-
…after canoeing and hiking for 2 WEEKS STRAIGHT!!
And he “WORKED THROUGH” the pain with stretching and ibuprofen while on his backpacking trip.
When he returned home, he had 9 sessions of physical therapy and then went on to backpack for another 2 weeks in the United States Continental Divide and had “0” back pain.
Superhuman?
Probably not.
Despite the growing field of research in injury assessment and risk management, there are quite a few unanswered questions. Standardization of measurements, sport-specific assessments, and more robust association in findings would help clear up many of these questions.
Practical application and programming for athletes and careers that require high fitness levels should also be discussed within the research community. Perhaps guidelines may help coaches develop pre-season injury assessments and provide strength and conditioning programs that are athlete-specific, essentially reducing the number of athletes sitting on the sidelines due to injury.
If you are an athlete or coach in Miami, FL and find this topic interesting, or want more information, reach out to our office for assistance.
In most situations conservative treatment is appropriate and is the best option.
Conservative treatment includes massage, chiropractic, physical therapy, exercise and even meditation.
If you do choose to seek non-surgical and non-medication based treatment, MRIs should be considered if the following are true:
Bacterial infections are often accompanied by a fever. So if you’ve been feverish for a month, have back pain and haven’t seen a doctor about that…
Go see one now!
Cauda equina syndrome is a life-threatening condition. If you show these signs and symptoms you should seek immediate medical attention.
NOTE TO THE READER: THIS BLOG POST DOES NOT OFFER ANY MEDICAL ADVICE.
IT IS FOR INFORMATIONAL PURPOSES ONLY.
YOUR SPECIFIC CASE NEEDS TO BE DISCUSSED WITH A QUALIFIED HEALTH CARE PROFESSIONAL.
If you have been treated by a chiropractor, massage therapist, physical therapist, have been exercising & following their advice AND you have not significantly improved for the past month, then it might be a good idea to consider seeking additional imaging or someone else to help.
For example, you’ve been up and down with the recovery but nothing seems to quite “stick” to improve how you feel.
Are you interested in learning more about MRIs and low back pain?
And maybe finding a solution to your back pain so you can enjoy beautiful Miami?
I want to share a story about two gentlemen:
The first patient: a 62 year old with two hip replacements, significant lumbar degenerative disc changes at multiple levels, osteophyte formation, and a retrolisthesis of L1-2 and L2-3.
The second patient: a 32 year old mechanic with a history of chronic low back pain, took off of work on disability with an MRI that was “relatively unremarkable” with some degenerative disc disease of L4-5 and L5-S1 and mild disc protrusion at L4-5.
No nerve impingement. No hip replacement surgery. No additional bony outgrowth.
Who would you think had more pain, the first or second man?
Mr. 62-year-old had one single episode of back pain 8 years after his bilateral hip replacement-
…after canoeing and hiking for 2 WEEKS STRAIGHT!!
And he “WORKED THROUGH” the pain with stretching and ibuprofen while on his backpacking trip.
When he returned home, he had 9 sessions of physical therapy and then went on to backpack for another 2 weeks in the United States Continental Divide and had “0” back pain.
Superhuman?
Probably not.
Despite the growing field of research in injury assessment and risk management, there are quite a few unanswered questions. Standardization of measurements, sport-specific assessments, and more robust association in findings would help clear up many of these questions.
Practical application and programming for athletes and careers that require high fitness levels should also be discussed within the research community. Perhaps guidelines may help coaches develop pre-season injury assessments and provide strength and conditioning programs that are athlete-specific, essentially reducing the number of athletes sitting on the sidelines due to injury.
If you are an athlete or coach in Miami, FL and find this topic interesting, or want more information, reach out to our office for assistance.
Non-specific low back pain: low back pain that is not due to a specific cause like a tumor, fracture, arthritis, herniated disc etc…
Neurological complications: numbness, tingling, altered sensation, weakness, muscular wasting or atrophy, abnormal reflexes
Spinal stenosis: narrowing of the spinal canal; can be due to herniated disc, fracture, bone spur
Radicular signs and symptoms: numbness, tingling in the buttocks, legs or feet
In most situations conservative treatment is appropriate and is the best option.
Conservative treatment includes massage, chiropractic, physical therapy, exercise and even meditation.
If you do choose to seek non-surgical and non-medication based treatment, MRIs should be considered if the following are true:
Bacterial infections are often accompanied by a fever. So if you’ve been feverish for a month, have back pain and haven’t seen a doctor about that…
Go see one now!
Cauda equina syndrome is a life-threatening condition. If you show these signs and symptoms you should seek immediate medical attention.
NOTE TO THE READER: THIS BLOG POST DOES NOT OFFER ANY MEDICAL ADVICE.
IT IS FOR INFORMATIONAL PURPOSES ONLY.
YOUR SPECIFIC CASE NEEDS TO BE DISCUSSED WITH A QUALIFIED HEALTH CARE PROFESSIONAL.
If you have been treated by a chiropractor, massage therapist, physical therapist, have been exercising & following their advice AND you have not significantly improved for the past month, then it might be a good idea to consider seeking additional imaging or someone else to help.
For example, you’ve been up and down with the recovery but nothing seems to quite “stick” to improve how you feel.
Are you interested in learning more about MRIs and low back pain?
And maybe finding a solution to your back pain so you can enjoy beautiful Miami?
I want to share a story about two gentlemen:
The first patient: a 62 year old with two hip replacements, significant lumbar degenerative disc changes at multiple levels, osteophyte formation, and a retrolisthesis of L1-2 and L2-3.
The second patient: a 32 year old mechanic with a history of chronic low back pain, took off of work on disability with an MRI that was “relatively unremarkable” with some degenerative disc disease of L4-5 and L5-S1 and mild disc protrusion at L4-5.
No nerve impingement. No hip replacement surgery. No additional bony outgrowth.
Who would you think had more pain, the first or second man?
Mr. 62-year-old had one single episode of back pain 8 years after his bilateral hip replacement-
…after canoeing and hiking for 2 WEEKS STRAIGHT!!
And he “WORKED THROUGH” the pain with stretching and ibuprofen while on his backpacking trip.
When he returned home, he had 9 sessions of physical therapy and then went on to backpack for another 2 weeks in the United States Continental Divide and had “0” back pain.
Superhuman?
Probably not.
Despite the growing field of research in injury assessment and risk management, there are quite a few unanswered questions. Standardization of measurements, sport-specific assessments, and more robust association in findings would help clear up many of these questions.
Practical application and programming for athletes and careers that require high fitness levels should also be discussed within the research community. Perhaps guidelines may help coaches develop pre-season injury assessments and provide strength and conditioning programs that are athlete-specific, essentially reducing the number of athletes sitting on the sidelines due to injury.
If you are an athlete or coach in Miami, FL and find this topic interesting, or want more information, reach out to our office for assistance.
Non-specific low back pain: low back pain that is not due to a specific cause like a tumor, fracture, arthritis, herniated disc etc…
Neurological complications: numbness, tingling, altered sensation, weakness, muscular wasting or atrophy, abnormal reflexes
Spinal stenosis: narrowing of the spinal canal; can be due to herniated disc, fracture, bone spur
Radicular signs and symptoms: numbness, tingling in the buttocks, legs or feet
In most situations conservative treatment is appropriate and is the best option.
Conservative treatment includes massage, chiropractic, physical therapy, exercise and even meditation.
If you do choose to seek non-surgical and non-medication based treatment, MRIs should be considered if the following are true:
Bacterial infections are often accompanied by a fever. So if you’ve been feverish for a month, have back pain and haven’t seen a doctor about that…
Go see one now!
Cauda equina syndrome is a life-threatening condition. If you show these signs and symptoms you should seek immediate medical attention.
NOTE TO THE READER: THIS BLOG POST DOES NOT OFFER ANY MEDICAL ADVICE.
IT IS FOR INFORMATIONAL PURPOSES ONLY.
YOUR SPECIFIC CASE NEEDS TO BE DISCUSSED WITH A QUALIFIED HEALTH CARE PROFESSIONAL.
If you have been treated by a chiropractor, massage therapist, physical therapist, have been exercising & following their advice AND you have not significantly improved for the past month, then it might be a good idea to consider seeking additional imaging or someone else to help.
For example, you’ve been up and down with the recovery but nothing seems to quite “stick” to improve how you feel.
Are you interested in learning more about MRIs and low back pain?
And maybe finding a solution to your back pain so you can enjoy beautiful Miami?
I want to share a story about two gentlemen:
The first patient: a 62 year old with two hip replacements, significant lumbar degenerative disc changes at multiple levels, osteophyte formation, and a retrolisthesis of L1-2 and L2-3.
The second patient: a 32 year old mechanic with a history of chronic low back pain, took off of work on disability with an MRI that was “relatively unremarkable” with some degenerative disc disease of L4-5 and L5-S1 and mild disc protrusion at L4-5.
No nerve impingement. No hip replacement surgery. No additional bony outgrowth.
Who would you think had more pain, the first or second man?
Mr. 62-year-old had one single episode of back pain 8 years after his bilateral hip replacement-
…after canoeing and hiking for 2 WEEKS STRAIGHT!!
And he “WORKED THROUGH” the pain with stretching and ibuprofen while on his backpacking trip.
When he returned home, he had 9 sessions of physical therapy and then went on to backpack for another 2 weeks in the United States Continental Divide and had “0” back pain.
Superhuman?
Probably not.
Despite the growing field of research in injury assessment and risk management, there are quite a few unanswered questions. Standardization of measurements, sport-specific assessments, and more robust association in findings would help clear up many of these questions.
Practical application and programming for athletes and careers that require high fitness levels should also be discussed within the research community. Perhaps guidelines may help coaches develop pre-season injury assessments and provide strength and conditioning programs that are athlete-specific, essentially reducing the number of athletes sitting on the sidelines due to injury.
If you are an athlete or coach in Miami, FL and find this topic interesting, or want more information, reach out to our office for assistance.
Here are the guidelines published by the American College of Physicians (ACP) and the American Pain Society (APS) for when it is appropriate to get an MRI.
These two organizations suggest MRIs should:
Non-specific low back pain: low back pain that is not due to a specific cause like a tumor, fracture, arthritis, herniated disc etc…
Neurological complications: numbness, tingling, altered sensation, weakness, muscular wasting or atrophy, abnormal reflexes
Spinal stenosis: narrowing of the spinal canal; can be due to herniated disc, fracture, bone spur
Radicular signs and symptoms: numbness, tingling in the buttocks, legs or feet
In most situations conservative treatment is appropriate and is the best option.
Conservative treatment includes massage, chiropractic, physical therapy, exercise and even meditation.
If you do choose to seek non-surgical and non-medication based treatment, MRIs should be considered if the following are true:
Bacterial infections are often accompanied by a fever. So if you’ve been feverish for a month, have back pain and haven’t seen a doctor about that…
Go see one now!
Cauda equina syndrome is a life-threatening condition. If you show these signs and symptoms you should seek immediate medical attention.
NOTE TO THE READER: THIS BLOG POST DOES NOT OFFER ANY MEDICAL ADVICE.
IT IS FOR INFORMATIONAL PURPOSES ONLY.
YOUR SPECIFIC CASE NEEDS TO BE DISCUSSED WITH A QUALIFIED HEALTH CARE PROFESSIONAL.
If you have been treated by a chiropractor, massage therapist, physical therapist, have been exercising & following their advice AND you have not significantly improved for the past month, then it might be a good idea to consider seeking additional imaging or someone else to help.
For example, you’ve been up and down with the recovery but nothing seems to quite “stick” to improve how you feel.
Are you interested in learning more about MRIs and low back pain?
And maybe finding a solution to your back pain so you can enjoy beautiful Miami?
I want to share a story about two gentlemen:
The first patient: a 62 year old with two hip replacements, significant lumbar degenerative disc changes at multiple levels, osteophyte formation, and a retrolisthesis of L1-2 and L2-3.
The second patient: a 32 year old mechanic with a history of chronic low back pain, took off of work on disability with an MRI that was “relatively unremarkable” with some degenerative disc disease of L4-5 and L5-S1 and mild disc protrusion at L4-5.
No nerve impingement. No hip replacement surgery. No additional bony outgrowth.
Who would you think had more pain, the first or second man?
Mr. 62-year-old had one single episode of back pain 8 years after his bilateral hip replacement-
…after canoeing and hiking for 2 WEEKS STRAIGHT!!
And he “WORKED THROUGH” the pain with stretching and ibuprofen while on his backpacking trip.
When he returned home, he had 9 sessions of physical therapy and then went on to backpack for another 2 weeks in the United States Continental Divide and had “0” back pain.
Superhuman?
Probably not.
Despite the growing field of research in injury assessment and risk management, there are quite a few unanswered questions. Standardization of measurements, sport-specific assessments, and more robust association in findings would help clear up many of these questions.
Practical application and programming for athletes and careers that require high fitness levels should also be discussed within the research community. Perhaps guidelines may help coaches develop pre-season injury assessments and provide strength and conditioning programs that are athlete-specific, essentially reducing the number of athletes sitting on the sidelines due to injury.
If you are an athlete or coach in Miami, FL and find this topic interesting, or want more information, reach out to our office for assistance.

Good, I’m glad we got that out of the way…
Here are the guidelines published by the American College of Physicians (ACP) and the American Pain Society (APS) for when it is appropriate to get an MRI.
These two organizations suggest MRIs should:
Non-specific low back pain: low back pain that is not due to a specific cause like a tumor, fracture, arthritis, herniated disc etc…
Neurological complications: numbness, tingling, altered sensation, weakness, muscular wasting or atrophy, abnormal reflexes
Spinal stenosis: narrowing of the spinal canal; can be due to herniated disc, fracture, bone spur
Radicular signs and symptoms: numbness, tingling in the buttocks, legs or feet
In most situations conservative treatment is appropriate and is the best option.
Conservative treatment includes massage, chiropractic, physical therapy, exercise and even meditation.
If you do choose to seek non-surgical and non-medication based treatment, MRIs should be considered if the following are true:
Bacterial infections are often accompanied by a fever. So if you’ve been feverish for a month, have back pain and haven’t seen a doctor about that…
Go see one now!
Cauda equina syndrome is a life-threatening condition. If you show these signs and symptoms you should seek immediate medical attention.
NOTE TO THE READER: THIS BLOG POST DOES NOT OFFER ANY MEDICAL ADVICE.
IT IS FOR INFORMATIONAL PURPOSES ONLY.
YOUR SPECIFIC CASE NEEDS TO BE DISCUSSED WITH A QUALIFIED HEALTH CARE PROFESSIONAL.
If you have been treated by a chiropractor, massage therapist, physical therapist, have been exercising & following their advice AND you have not significantly improved for the past month, then it might be a good idea to consider seeking additional imaging or someone else to help.
For example, you’ve been up and down with the recovery but nothing seems to quite “stick” to improve how you feel.
Are you interested in learning more about MRIs and low back pain?
And maybe finding a solution to your back pain so you can enjoy beautiful Miami?
I want to share a story about two gentlemen:
The first patient: a 62 year old with two hip replacements, significant lumbar degenerative disc changes at multiple levels, osteophyte formation, and a retrolisthesis of L1-2 and L2-3.
The second patient: a 32 year old mechanic with a history of chronic low back pain, took off of work on disability with an MRI that was “relatively unremarkable” with some degenerative disc disease of L4-5 and L5-S1 and mild disc protrusion at L4-5.
No nerve impingement. No hip replacement surgery. No additional bony outgrowth.
Who would you think had more pain, the first or second man?
Mr. 62-year-old had one single episode of back pain 8 years after his bilateral hip replacement-
…after canoeing and hiking for 2 WEEKS STRAIGHT!!
And he “WORKED THROUGH” the pain with stretching and ibuprofen while on his backpacking trip.
When he returned home, he had 9 sessions of physical therapy and then went on to backpack for another 2 weeks in the United States Continental Divide and had “0” back pain.
Superhuman?
Probably not.
Despite the growing field of research in injury assessment and risk management, there are quite a few unanswered questions. Standardization of measurements, sport-specific assessments, and more robust association in findings would help clear up many of these questions.
Practical application and programming for athletes and careers that require high fitness levels should also be discussed within the research community. Perhaps guidelines may help coaches develop pre-season injury assessments and provide strength and conditioning programs that are athlete-specific, essentially reducing the number of athletes sitting on the sidelines due to injury.
If you are an athlete or coach in Miami, FL and find this topic interesting, or want more information, reach out to our office for assistance.
To better answer WHEN would be a good time to have an MRI, we need to understand a little background info.
Good, I’m glad we got that out of the way…
Here are the guidelines published by the American College of Physicians (ACP) and the American Pain Society (APS) for when it is appropriate to get an MRI.
These two organizations suggest MRIs should:
Non-specific low back pain: low back pain that is not due to a specific cause like a tumor, fracture, arthritis, herniated disc etc…
Neurological complications: numbness, tingling, altered sensation, weakness, muscular wasting or atrophy, abnormal reflexes
Spinal stenosis: narrowing of the spinal canal; can be due to herniated disc, fracture, bone spur
Radicular signs and symptoms: numbness, tingling in the buttocks, legs or feet
In most situations conservative treatment is appropriate and is the best option.
Conservative treatment includes massage, chiropractic, physical therapy, exercise and even meditation.
If you do choose to seek non-surgical and non-medication based treatment, MRIs should be considered if the following are true:
Bacterial infections are often accompanied by a fever. So if you’ve been feverish for a month, have back pain and haven’t seen a doctor about that…
Go see one now!
Cauda equina syndrome is a life-threatening condition. If you show these signs and symptoms you should seek immediate medical attention.
NOTE TO THE READER: THIS BLOG POST DOES NOT OFFER ANY MEDICAL ADVICE.
IT IS FOR INFORMATIONAL PURPOSES ONLY.
YOUR SPECIFIC CASE NEEDS TO BE DISCUSSED WITH A QUALIFIED HEALTH CARE PROFESSIONAL.
If you have been treated by a chiropractor, massage therapist, physical therapist, have been exercising & following their advice AND you have not significantly improved for the past month, then it might be a good idea to consider seeking additional imaging or someone else to help.
For example, you’ve been up and down with the recovery but nothing seems to quite “stick” to improve how you feel.
Are you interested in learning more about MRIs and low back pain?
And maybe finding a solution to your back pain so you can enjoy beautiful Miami?
I want to share a story about two gentlemen:
The first patient: a 62 year old with two hip replacements, significant lumbar degenerative disc changes at multiple levels, osteophyte formation, and a retrolisthesis of L1-2 and L2-3.
The second patient: a 32 year old mechanic with a history of chronic low back pain, took off of work on disability with an MRI that was “relatively unremarkable” with some degenerative disc disease of L4-5 and L5-S1 and mild disc protrusion at L4-5.
No nerve impingement. No hip replacement surgery. No additional bony outgrowth.
Who would you think had more pain, the first or second man?
Mr. 62-year-old had one single episode of back pain 8 years after his bilateral hip replacement-
…after canoeing and hiking for 2 WEEKS STRAIGHT!!
And he “WORKED THROUGH” the pain with stretching and ibuprofen while on his backpacking trip.
When he returned home, he had 9 sessions of physical therapy and then went on to backpack for another 2 weeks in the United States Continental Divide and had “0” back pain.
Superhuman?
Probably not.
Despite the growing field of research in injury assessment and risk management, there are quite a few unanswered questions. Standardization of measurements, sport-specific assessments, and more robust association in findings would help clear up many of these questions.
Practical application and programming for athletes and careers that require high fitness levels should also be discussed within the research community. Perhaps guidelines may help coaches develop pre-season injury assessments and provide strength and conditioning programs that are athlete-specific, essentially reducing the number of athletes sitting on the sidelines due to injury.
If you are an athlete or coach in Miami, FL and find this topic interesting, or want more information, reach out to our office for assistance.