Patella stress fractures should be treated with a 4-6 week period of immobilization in a long leg cast. Healing time is typically faster in youth compared to adults. A displaced fracture or nonunion fracture should be referred to an orthopedic surgeon.
Tibial stress fractures have a high risk of nonunion. The “dreaded black line” may be observed on x-rays. If x-rays do not demonstrate a defect, MRI or CT scan may be warranted. Treatment requires a period of non-weightbearing and progressive return to sport. If nonoperative treatment fails, surgical intervention may be necessary.
Ankle stress fractures are uncommon in youth athletes. They are generally treated with rest and gradual return to sport. Stress fractures of the ankle are more common in bounding/jumping sports including gymnastics and dance. If the fracture progresses, surgical intervention may be required.
Tarsal stress fractures are most prevalent in track and field, football and soccer. The most reliable method of identifying this type of fracture is a CT scan. There may be a delay in proper treatment due to the vague nature of complaints from the youth athlete. Poorly fitting footwear may contribute to the development and subsequent aggravation of the fracture.
Parents, coaches, athletes and health care providers should have a high index of suspicion when pain is reported at the site of high risk bone injuries. Localized tenderness over the site, coupled with the athletes history of onset of pain, should warrant imaging by a health care practitioner. Tenderness to touch of the spine and hip may not be reliable, thus, imaging should be done to rule out bony injury.
Radiographs (x-rays) may not be sensitive enough to identify stress reactions/fractures. Further imaging may be necessary (MRI, CT scan) to rule out bone injuries in youth athletes. Treatment of high risk stress reactions and fractures are specific to the site of injury. Very often, a period of rest (non-weightbearing) is required to allow the bone to heal. A progressive and graded return to sport may help prevent subsequent injury.
While there are no studies specific to prevention of stress fractures in youth athletes, the general consensus is similar to adults. Limiting high impact activities, optimizing vitamin D and calcium intake, screening for the female athlete triad and proper footwear should be assessed. Early recognition is key to optimal treatment.
If you are a youth athlete, parent of a youth athlete or coach youth athletics in Miami, Florida and have questions about information presented in this post, give our office a call. We offers seminars to educate the community on best practices for keeping youth athletes participating in sport. As a lifelong athlete myself, I can appreciate the time, effort and role parents and coaches can play in the development of their children. My goal is to keep as many people participating in athletics for as long as possible.
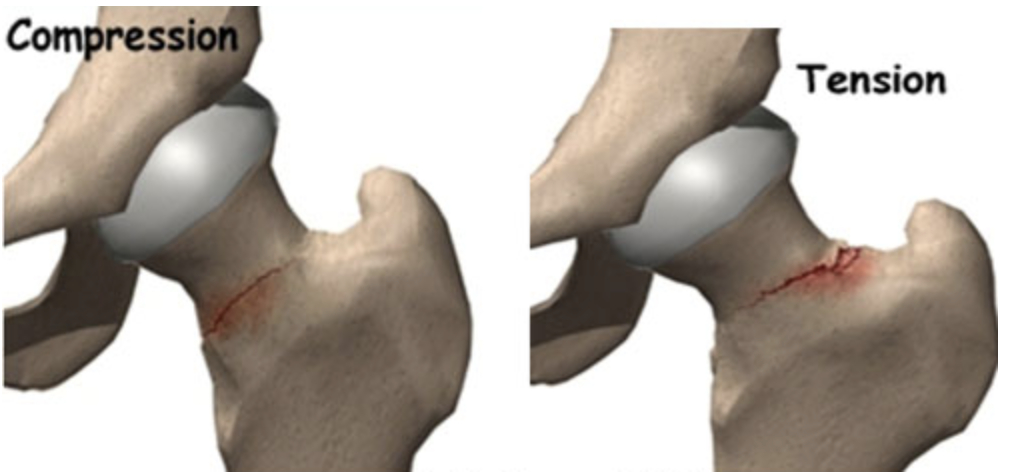
While stress fractures of the femoral neck are not common in children and adolescents, if not recognized early and treated, complete fracture may occur. If an athlete is complaining of hip or groin pain in the front, the health care provider, coach and parent should be highly suspicious. Depending on the location of the fracture, referral to an orthopedic surgeon is necessary. A period of non-weightbearing may be required to allow the bone to heal.
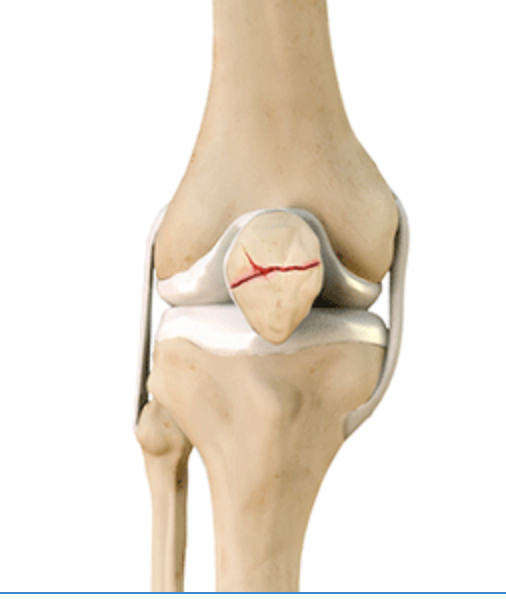
Patella stress fractures should be treated with a 4-6 week period of immobilization in a long leg cast. Healing time is typically faster in youth compared to adults. A displaced fracture or nonunion fracture should be referred to an orthopedic surgeon.
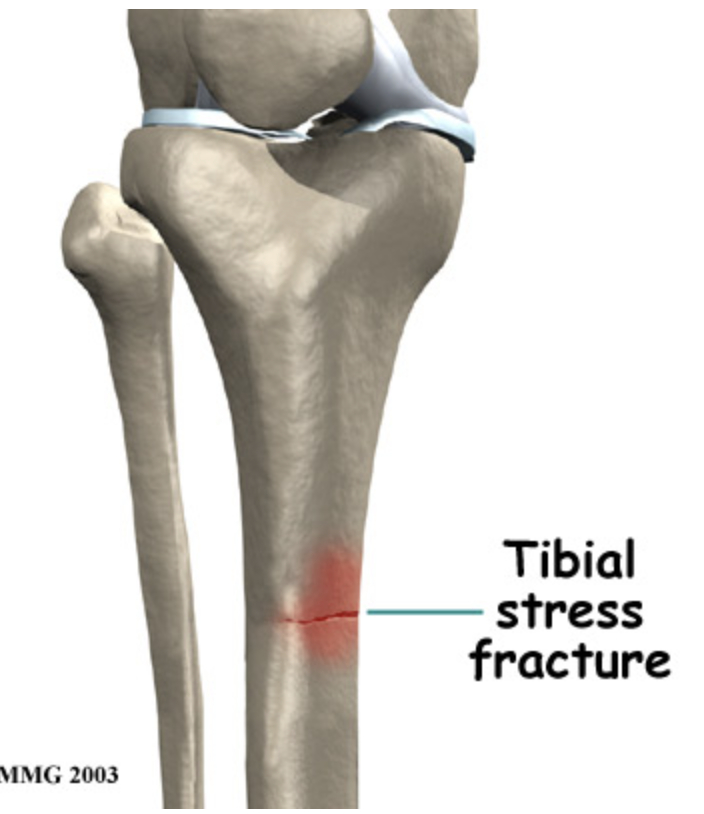
Tibial stress fractures have a high risk of nonunion. The “dreaded black line” may be observed on x-rays. If x-rays do not demonstrate a defect, MRI or CT scan may be warranted. Treatment requires a period of non-weightbearing and progressive return to sport. If nonoperative treatment fails, surgical intervention may be necessary.
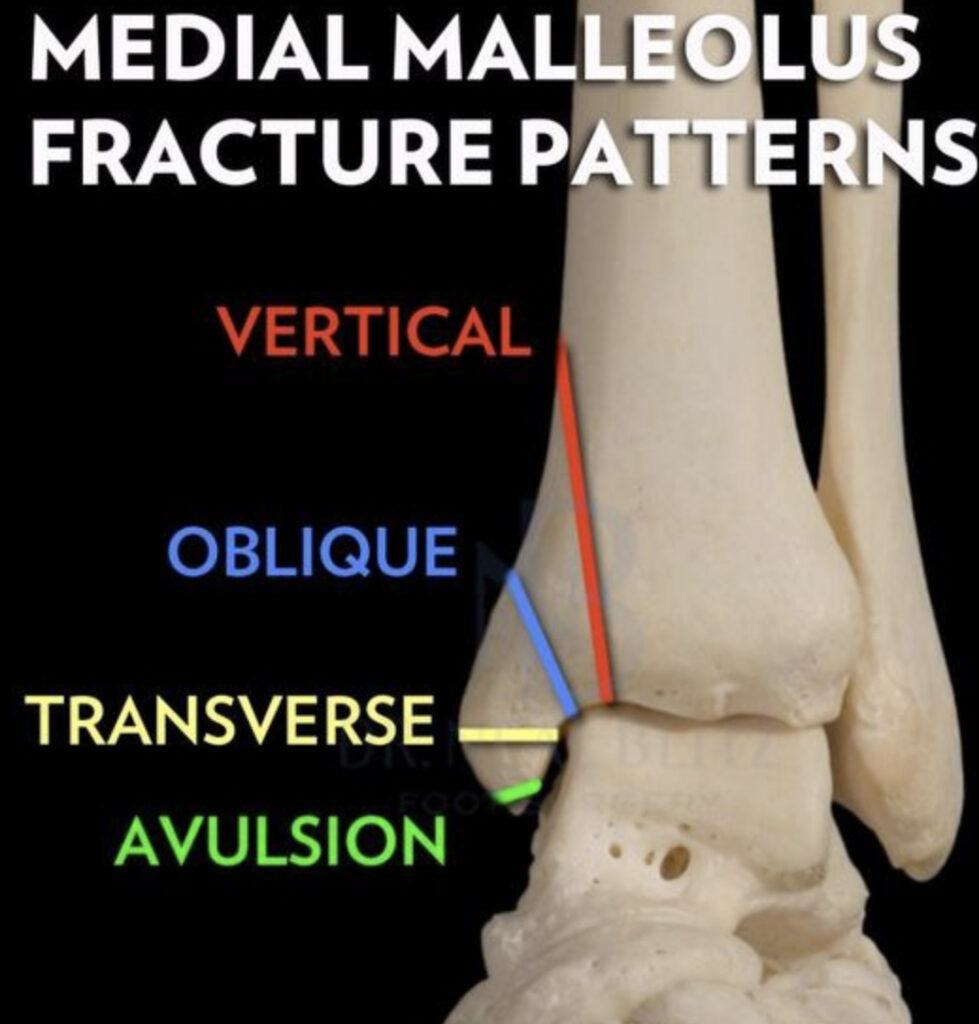
Ankle stress fractures are uncommon in youth athletes. They are generally treated with rest and gradual return to sport. Stress fractures of the ankle are more common in bounding/jumping sports including gymnastics and dance. If the fracture progresses, surgical intervention may be required.
Tarsal stress fractures are most prevalent in track and field, football and soccer. The most reliable method of identifying this type of fracture is a CT scan. There may be a delay in proper treatment due to the vague nature of complaints from the youth athlete. Poorly fitting footwear may contribute to the development and subsequent aggravation of the fracture.
Parents, coaches, athletes and health care providers should have a high index of suspicion when pain is reported at the site of high risk bone injuries. Localized tenderness over the site, coupled with the athletes history of onset of pain, should warrant imaging by a health care practitioner. Tenderness to touch of the spine and hip may not be reliable, thus, imaging should be done to rule out bony injury.
Radiographs (x-rays) may not be sensitive enough to identify stress reactions/fractures. Further imaging may be necessary (MRI, CT scan) to rule out bone injuries in youth athletes. Treatment of high risk stress reactions and fractures are specific to the site of injury. Very often, a period of rest (non-weightbearing) is required to allow the bone to heal. A progressive and graded return to sport may help prevent subsequent injury.
While there are no studies specific to prevention of stress fractures in youth athletes, the general consensus is similar to adults. Limiting high impact activities, optimizing vitamin D and calcium intake, screening for the female athlete triad and proper footwear should be assessed. Early recognition is key to optimal treatment.
If you are a youth athlete, parent of a youth athlete or coach youth athletics in Miami, Florida and have questions about information presented in this post, give our office a call. We offers seminars to educate the community on best practices for keeping youth athletes participating in sport. As a lifelong athlete myself, I can appreciate the time, effort and role parents and coaches can play in the development of their children. My goal is to keep as many people participating in athletics for as long as possible.
About half of youth athletes evaluated for low back pain presented with occult spondylosis. Nonunion of the bone ranged between 14-70%, with those being untreated being more likely to experience nonunion. On average, about 5.4 months off from sport was required for bone healing. This typically included bracing, but an individual approach best determines which intervention is necessary. Surgical pars repair (fusion) may be necessary if no union is demonstrated at 6 months.
While stress fractures of the femoral neck are not common in children and adolescents, if not recognized early and treated, complete fracture may occur. If an athlete is complaining of hip or groin pain in the front, the health care provider, coach and parent should be highly suspicious. Depending on the location of the fracture, referral to an orthopedic surgeon is necessary. A period of non-weightbearing may be required to allow the bone to heal.
Patella stress fractures should be treated with a 4-6 week period of immobilization in a long leg cast. Healing time is typically faster in youth compared to adults. A displaced fracture or nonunion fracture should be referred to an orthopedic surgeon.
Tibial stress fractures have a high risk of nonunion. The “dreaded black line” may be observed on x-rays. If x-rays do not demonstrate a defect, MRI or CT scan may be warranted. Treatment requires a period of non-weightbearing and progressive return to sport. If nonoperative treatment fails, surgical intervention may be necessary.
Ankle stress fractures are uncommon in youth athletes. They are generally treated with rest and gradual return to sport. Stress fractures of the ankle are more common in bounding/jumping sports including gymnastics and dance. If the fracture progresses, surgical intervention may be required.
Tarsal stress fractures are most prevalent in track and field, football and soccer. The most reliable method of identifying this type of fracture is a CT scan. There may be a delay in proper treatment due to the vague nature of complaints from the youth athlete. Poorly fitting footwear may contribute to the development and subsequent aggravation of the fracture.
Parents, coaches, athletes and health care providers should have a high index of suspicion when pain is reported at the site of high risk bone injuries. Localized tenderness over the site, coupled with the athletes history of onset of pain, should warrant imaging by a health care practitioner. Tenderness to touch of the spine and hip may not be reliable, thus, imaging should be done to rule out bony injury.
Radiographs (x-rays) may not be sensitive enough to identify stress reactions/fractures. Further imaging may be necessary (MRI, CT scan) to rule out bone injuries in youth athletes. Treatment of high risk stress reactions and fractures are specific to the site of injury. Very often, a period of rest (non-weightbearing) is required to allow the bone to heal. A progressive and graded return to sport may help prevent subsequent injury.
While there are no studies specific to prevention of stress fractures in youth athletes, the general consensus is similar to adults. Limiting high impact activities, optimizing vitamin D and calcium intake, screening for the female athlete triad and proper footwear should be assessed. Early recognition is key to optimal treatment.
If you are a youth athlete, parent of a youth athlete or coach youth athletics in Miami, Florida and have questions about information presented in this post, give our office a call. We offers seminars to educate the community on best practices for keeping youth athletes participating in sport. As a lifelong athlete myself, I can appreciate the time, effort and role parents and coaches can play in the development of their children. My goal is to keep as many people participating in athletics for as long as possible.
While most stress fractures heal with appropriate rest, rehabilitation and progressive return to sport, certain stress reactions or fractures do not heal readily. These are deemed “high risk”. Improper identification and treatment can lead to nonunion, chronic pain or lead to degenerative joint disease. Delayed union has been reported to occur in up to 10% of athletic stress fractures.
About half of youth athletes evaluated for low back pain presented with occult spondylosis. Nonunion of the bone ranged between 14-70%, with those being untreated being more likely to experience nonunion. On average, about 5.4 months off from sport was required for bone healing. This typically included bracing, but an individual approach best determines which intervention is necessary. Surgical pars repair (fusion) may be necessary if no union is demonstrated at 6 months.
While stress fractures of the femoral neck are not common in children and adolescents, if not recognized early and treated, complete fracture may occur. If an athlete is complaining of hip or groin pain in the front, the health care provider, coach and parent should be highly suspicious. Depending on the location of the fracture, referral to an orthopedic surgeon is necessary. A period of non-weightbearing may be required to allow the bone to heal.
Patella stress fractures should be treated with a 4-6 week period of immobilization in a long leg cast. Healing time is typically faster in youth compared to adults. A displaced fracture or nonunion fracture should be referred to an orthopedic surgeon.
Tibial stress fractures have a high risk of nonunion. The “dreaded black line” may be observed on x-rays. If x-rays do not demonstrate a defect, MRI or CT scan may be warranted. Treatment requires a period of non-weightbearing and progressive return to sport. If nonoperative treatment fails, surgical intervention may be necessary.
Ankle stress fractures are uncommon in youth athletes. They are generally treated with rest and gradual return to sport. Stress fractures of the ankle are more common in bounding/jumping sports including gymnastics and dance. If the fracture progresses, surgical intervention may be required.
Tarsal stress fractures are most prevalent in track and field, football and soccer. The most reliable method of identifying this type of fracture is a CT scan. There may be a delay in proper treatment due to the vague nature of complaints from the youth athlete. Poorly fitting footwear may contribute to the development and subsequent aggravation of the fracture.
Parents, coaches, athletes and health care providers should have a high index of suspicion when pain is reported at the site of high risk bone injuries. Localized tenderness over the site, coupled with the athletes history of onset of pain, should warrant imaging by a health care practitioner. Tenderness to touch of the spine and hip may not be reliable, thus, imaging should be done to rule out bony injury.
Radiographs (x-rays) may not be sensitive enough to identify stress reactions/fractures. Further imaging may be necessary (MRI, CT scan) to rule out bone injuries in youth athletes. Treatment of high risk stress reactions and fractures are specific to the site of injury. Very often, a period of rest (non-weightbearing) is required to allow the bone to heal. A progressive and graded return to sport may help prevent subsequent injury.
While there are no studies specific to prevention of stress fractures in youth athletes, the general consensus is similar to adults. Limiting high impact activities, optimizing vitamin D and calcium intake, screening for the female athlete triad and proper footwear should be assessed. Early recognition is key to optimal treatment.
If you are a youth athlete, parent of a youth athlete or coach youth athletics in Miami, Florida and have questions about information presented in this post, give our office a call. We offers seminars to educate the community on best practices for keeping youth athletes participating in sport. As a lifelong athlete myself, I can appreciate the time, effort and role parents and coaches can play in the development of their children. My goal is to keep as many people participating in athletics for as long as possible.
High risk overuse injuries in youth athletes may be exacerbated if they are unrecognized or inappropriately treated. This can lead to significant time off from sport and threaten future participation. High risk injuries include stress fractures, physeal stress injuries, osteochondritis dessicans, some apophyseal injuries and effort thrombosis.
Let’s take a look at these in further detail.
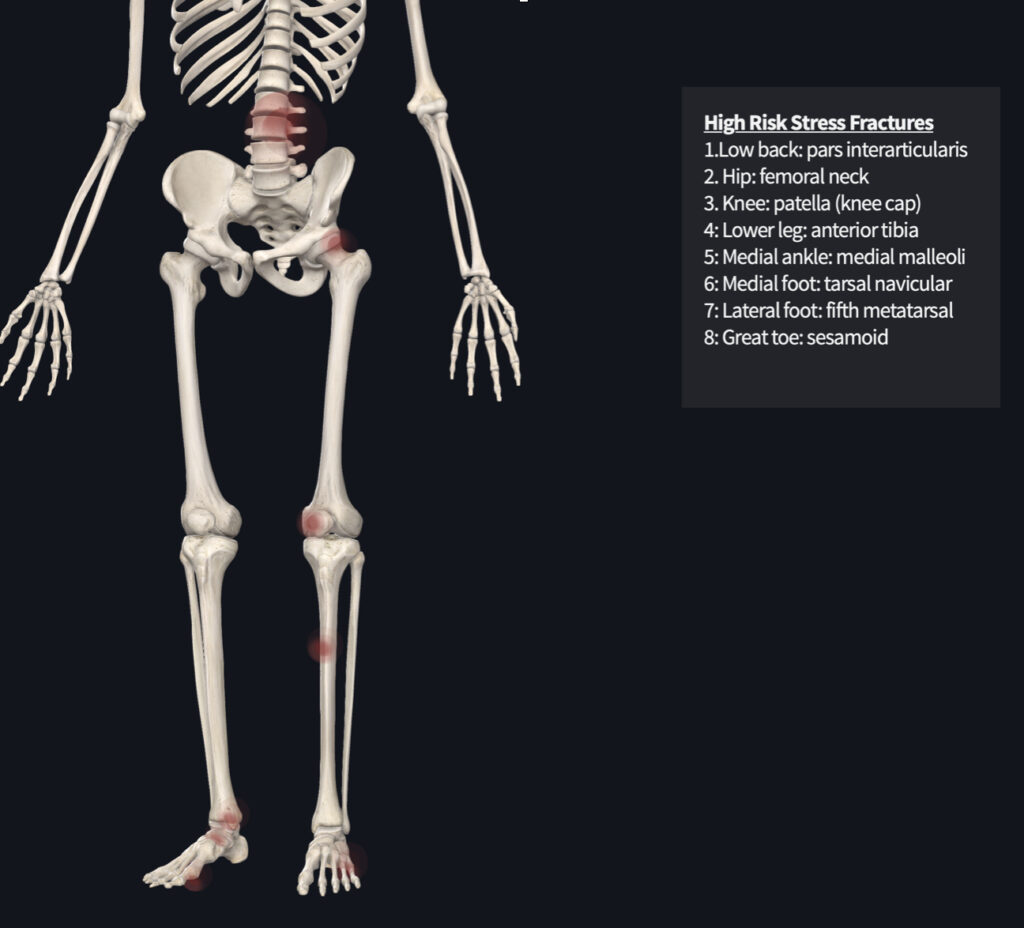
While most stress fractures heal with appropriate rest, rehabilitation and progressive return to sport, certain stress reactions or fractures do not heal readily. These are deemed “high risk”. Improper identification and treatment can lead to nonunion, chronic pain or lead to degenerative joint disease. Delayed union has been reported to occur in up to 10% of athletic stress fractures.
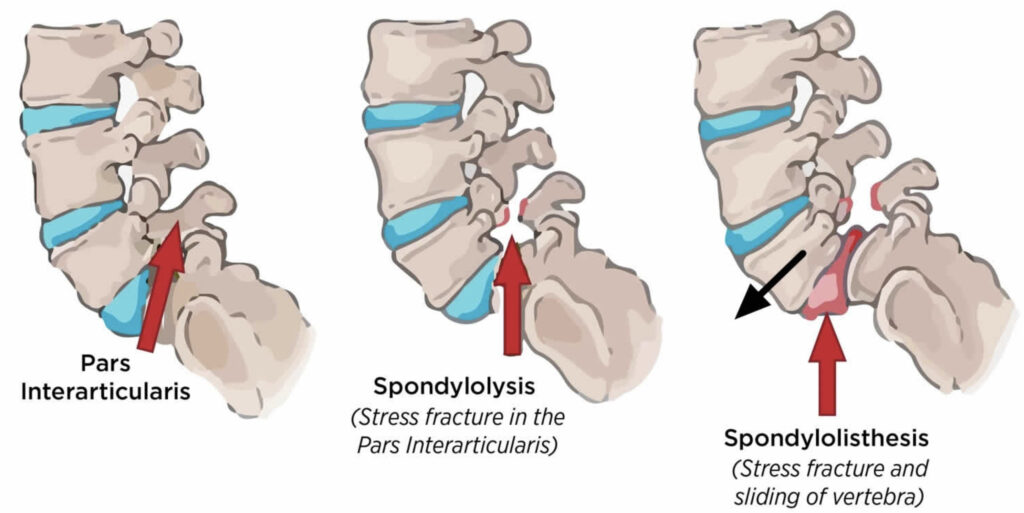
About half of youth athletes evaluated for low back pain presented with occult spondylosis. Nonunion of the bone ranged between 14-70%, with those being untreated being more likely to experience nonunion. On average, about 5.4 months off from sport was required for bone healing. This typically included bracing, but an individual approach best determines which intervention is necessary. Surgical pars repair (fusion) may be necessary if no union is demonstrated at 6 months.
While stress fractures of the femoral neck are not common in children and adolescents, if not recognized early and treated, complete fracture may occur. If an athlete is complaining of hip or groin pain in the front, the health care provider, coach and parent should be highly suspicious. Depending on the location of the fracture, referral to an orthopedic surgeon is necessary. A period of non-weightbearing may be required to allow the bone to heal.
Patella stress fractures should be treated with a 4-6 week period of immobilization in a long leg cast. Healing time is typically faster in youth compared to adults. A displaced fracture or nonunion fracture should be referred to an orthopedic surgeon.
Tibial stress fractures have a high risk of nonunion. The “dreaded black line” may be observed on x-rays. If x-rays do not demonstrate a defect, MRI or CT scan may be warranted. Treatment requires a period of non-weightbearing and progressive return to sport. If nonoperative treatment fails, surgical intervention may be necessary.
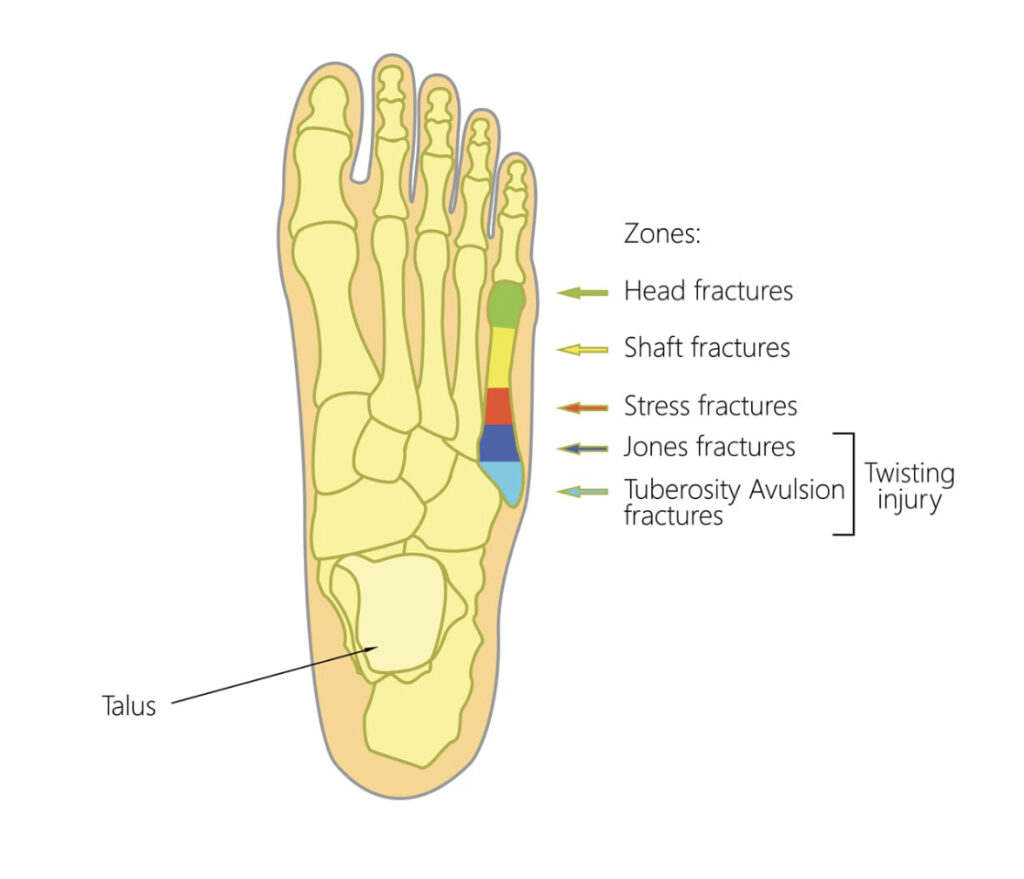
Ankle stress fractures are uncommon in youth athletes. They are generally treated with rest and gradual return to sport. Stress fractures of the ankle are more common in bounding/jumping sports including gymnastics and dance. If the fracture progresses, surgical intervention may be required.
Tarsal stress fractures are most prevalent in track and field, football and soccer. The most reliable method of identifying this type of fracture is a CT scan. There may be a delay in proper treatment due to the vague nature of complaints from the youth athlete. Poorly fitting footwear may contribute to the development and subsequent aggravation of the fracture.
Parents, coaches, athletes and health care providers should have a high index of suspicion when pain is reported at the site of high risk bone injuries. Localized tenderness over the site, coupled with the athletes history of onset of pain, should warrant imaging by a health care practitioner. Tenderness to touch of the spine and hip may not be reliable, thus, imaging should be done to rule out bony injury.
Radiographs (x-rays) may not be sensitive enough to identify stress reactions/fractures. Further imaging may be necessary (MRI, CT scan) to rule out bone injuries in youth athletes. Treatment of high risk stress reactions and fractures are specific to the site of injury. Very often, a period of rest (non-weightbearing) is required to allow the bone to heal. A progressive and graded return to sport may help prevent subsequent injury.
While there are no studies specific to prevention of stress fractures in youth athletes, the general consensus is similar to adults. Limiting high impact activities, optimizing vitamin D and calcium intake, screening for the female athlete triad and proper footwear should be assessed. Early recognition is key to optimal treatment.
If you are a youth athlete, parent of a youth athlete or coach youth athletics in Miami, Florida and have questions about information presented in this post, give our office a call. We offers seminars to educate the community on best practices for keeping youth athletes participating in sport. As a lifelong athlete myself, I can appreciate the time, effort and role parents and coaches can play in the development of their children. My goal is to keep as many people participating in athletics for as long as possible.