Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
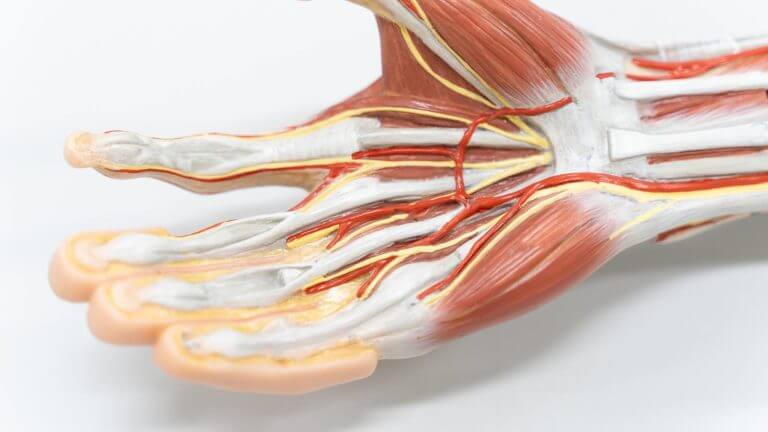
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
The distal row (on the underside of your wrist closest to your palm) includes the:
Trapezium
Trapezoid
Capitate
Hamate
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
The distal row (on the underside of your wrist closest to your palm) includes the:
Trapezium
Trapezoid
Capitate
Hamate
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Your wrist is a complex joint made of eight bones that are arranged into two rows.
The proximal row (on the back of your hand, closest to your forearm) includes the:
Scaphoid
Lunate
Triquetrum
Pisiform
The distal row (on the underside of your wrist closest to your palm) includes the:
Trapezium
Trapezoid
Capitate
Hamate
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Metacarpals: The bones that are in your palm and give it its shape
Phalanges: The individual bones that make up the segments of your fingers and thumb
Sesamoids: Small bones embedded in your tendons that help them move smoothly
Wrist bones
Your wrist is a complex joint made of eight bones that are arranged into two rows.
The proximal row (on the back of your hand, closest to your forearm) includes the:
Scaphoid
Lunate
Triquetrum
Pisiform
The distal row (on the underside of your wrist closest to your palm) includes the:
Trapezium
Trapezoid
Capitate
Hamate
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
There are 19 bones in each of your hands. They’re grouped together by their location and function:
Metacarpals: The bones that are in your palm and give it its shape
Phalanges: The individual bones that make up the segments of your fingers and thumb
Sesamoids: Small bones embedded in your tendons that help them move smoothly
Wrist bones
Your wrist is a complex joint made of eight bones that are arranged into two rows.
The proximal row (on the back of your hand, closest to your forearm) includes the:
Scaphoid
Lunate
Triquetrum
Pisiform
The distal row (on the underside of your wrist closest to your palm) includes the:
Trapezium
Trapezoid
Capitate
Hamate
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Bones provide the main structural support in your hand and wrist. They give them their shape and are the anchors other pieces are connected to.
Hand bones
There are 19 bones in each of your hands. They’re grouped together by their location and function:
Metacarpals: The bones that are in your palm and give it its shape
Phalanges: The individual bones that make up the segments of your fingers and thumb
Sesamoids: Small bones embedded in your tendons that help them move smoothly
Wrist bones
Your wrist is a complex joint made of eight bones that are arranged into two rows.
The proximal row (on the back of your hand, closest to your forearm) includes the:
Scaphoid
Lunate
Triquetrum
Pisiform
The distal row (on the underside of your wrist closest to your palm) includes the:
Trapezium
Trapezoid
Capitate
Hamate
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Bones provide the main structural support in your hand and wrist. They give them their shape and are the anchors other pieces are connected to.
Hand bones
There are 19 bones in each of your hands. They’re grouped together by their location and function:
Metacarpals: The bones that are in your palm and give it its shape
Phalanges: The individual bones that make up the segments of your fingers and thumb
Sesamoids: Small bones embedded in your tendons that help them move smoothly
Wrist bones
Your wrist is a complex joint made of eight bones that are arranged into two rows.
The proximal row (on the back of your hand, closest to your forearm) includes the:
Scaphoid
Lunate
Triquetrum
Pisiform
The distal row (on the underside of your wrist closest to your palm) includes the:
Trapezium
Trapezoid
Capitate
Hamate
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
The parts that make up your hand and wrist are layered upon each other to form a three-dimensional shape that gives them the ability to move and function.
Your hand and wrist are made of:
Bones.
Muscles
Nerves
Tendons
Ligaments
Blood vessels (arteries and veins)
Lymphatic vessels
Hand and wrist bones
Bones provide the main structural support in your hand and wrist. They give them their shape and are the anchors other pieces are connected to.
Hand bones
There are 19 bones in each of your hands. They’re grouped together by their location and function:
Metacarpals: The bones that are in your palm and give it its shape
Phalanges: The individual bones that make up the segments of your fingers and thumb
Sesamoids: Small bones embedded in your tendons that help them move smoothly
Wrist bones
Your wrist is a complex joint made of eight bones that are arranged into two rows.
The proximal row (on the back of your hand, closest to your forearm) includes the:
Scaphoid
Lunate
Triquetrum
Pisiform
The distal row (on the underside of your wrist closest to your palm) includes the:
Trapezium
Trapezoid
Capitate
Hamate
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Your hand and wrist are structured to allow you to move, flex and rotate your wrist joint and to use your hand to grab and touch objects.
Your wrist acts like a pivot point that can move in almost any direction as you reach and flex your hand. Think about your hand and wrist like a crane game at an arcade. Your hand is the claw that grabs and holds prizes, and your wrist is the mechanical joint that lets the claw move up and down, and side to side.
Hand and wrist anatomy
The parts that make up your hand and wrist are layered upon each other to form a three-dimensional shape that gives them the ability to move and function.
Your hand and wrist are made of:
Bones.
Muscles
Nerves
Tendons
Ligaments
Blood vessels (arteries and veins)
Lymphatic vessels
Hand and wrist bones
Bones provide the main structural support in your hand and wrist. They give them their shape and are the anchors other pieces are connected to.
Hand bones
There are 19 bones in each of your hands. They’re grouped together by their location and function:
Metacarpals: The bones that are in your palm and give it its shape
Phalanges: The individual bones that make up the segments of your fingers and thumb
Sesamoids: Small bones embedded in your tendons that help them move smoothly
Wrist bones
Your wrist is a complex joint made of eight bones that are arranged into two rows.
The proximal row (on the back of your hand, closest to your forearm) includes the:
Scaphoid
Lunate
Triquetrum
Pisiform
The distal row (on the underside of your wrist closest to your palm) includes the:
Trapezium
Trapezoid
Capitate
Hamate
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Your wrist is the joint at the end of your forearm. It’s the hinge between your arm and hand that lets you reposition your hand.
Your hand begins where your wrist ends. It includes your palm, fingers and thumb.
How are the hand and wrist structured?
Your hand and wrist are structured to allow you to move, flex and rotate your wrist joint and to use your hand to grab and touch objects.
Your wrist acts like a pivot point that can move in almost any direction as you reach and flex your hand. Think about your hand and wrist like a crane game at an arcade. Your hand is the claw that grabs and holds prizes, and your wrist is the mechanical joint that lets the claw move up and down, and side to side.
Hand and wrist anatomy
The parts that make up your hand and wrist are layered upon each other to form a three-dimensional shape that gives them the ability to move and function.
Your hand and wrist are made of:
Bones.
Muscles
Nerves
Tendons
Ligaments
Blood vessels (arteries and veins)
Lymphatic vessels
Hand and wrist bones
Bones provide the main structural support in your hand and wrist. They give them their shape and are the anchors other pieces are connected to.
Hand bones
There are 19 bones in each of your hands. They’re grouped together by their location and function:
Metacarpals: The bones that are in your palm and give it its shape
Phalanges: The individual bones that make up the segments of your fingers and thumb
Sesamoids: Small bones embedded in your tendons that help them move smoothly
Wrist bones
Your wrist is a complex joint made of eight bones that are arranged into two rows.
The proximal row (on the back of your hand, closest to your forearm) includes the:
Scaphoid
Lunate
Triquetrum
Pisiform
The distal row (on the underside of your wrist closest to your palm) includes the:
Trapezium
Trapezoid
Capitate
Hamate
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Your hand and wrist help you interact with the world around you. They’re probably the first body part that comes to mind when you think about your sense of touch.
They help you do everything throughout your day that involves touching, holding or using something with your fingers.
Where are the hand and wrist located?
Your wrist is the joint at the end of your forearm. It’s the hinge between your arm and hand that lets you reposition your hand.
Your hand begins where your wrist ends. It includes your palm, fingers and thumb.
How are the hand and wrist structured?
Your hand and wrist are structured to allow you to move, flex and rotate your wrist joint and to use your hand to grab and touch objects.
Your wrist acts like a pivot point that can move in almost any direction as you reach and flex your hand. Think about your hand and wrist like a crane game at an arcade. Your hand is the claw that grabs and holds prizes, and your wrist is the mechanical joint that lets the claw move up and down, and side to side.
Hand and wrist anatomy
The parts that make up your hand and wrist are layered upon each other to form a three-dimensional shape that gives them the ability to move and function.
Your hand and wrist are made of:
Bones.
Muscles
Nerves
Tendons
Ligaments
Blood vessels (arteries and veins)
Lymphatic vessels
Hand and wrist bones
Bones provide the main structural support in your hand and wrist. They give them their shape and are the anchors other pieces are connected to.
Hand bones
There are 19 bones in each of your hands. They’re grouped together by their location and function:
Metacarpals: The bones that are in your palm and give it its shape
Phalanges: The individual bones that make up the segments of your fingers and thumb
Sesamoids: Small bones embedded in your tendons that help them move smoothly
Wrist bones
Your wrist is a complex joint made of eight bones that are arranged into two rows.
The proximal row (on the back of your hand, closest to your forearm) includes the:
Scaphoid
Lunate
Triquetrum
Pisiform
The distal row (on the underside of your wrist closest to your palm) includes the:
Trapezium
Trapezoid
Capitate
Hamate
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Your hand and wrist are complex parts of your body that let you touch and control objects.
They’re a complicated network of bones, muscles, nerves tendons and ligaments, blood vessels and parts of your lymphatic system.
What do the hand and wrist do?
Your hand and wrist help you interact with the world around you. They’re probably the first body part that comes to mind when you think about your sense of touch.
They help you do everything throughout your day that involves touching, holding or using something with your fingers.
Where are the hand and wrist located?
Your wrist is the joint at the end of your forearm. It’s the hinge between your arm and hand that lets you reposition your hand.
Your hand begins where your wrist ends. It includes your palm, fingers and thumb.
How are the hand and wrist structured?
Your hand and wrist are structured to allow you to move, flex and rotate your wrist joint and to use your hand to grab and touch objects.
Your wrist acts like a pivot point that can move in almost any direction as you reach and flex your hand. Think about your hand and wrist like a crane game at an arcade. Your hand is the claw that grabs and holds prizes, and your wrist is the mechanical joint that lets the claw move up and down, and side to side.
Hand and wrist anatomy
The parts that make up your hand and wrist are layered upon each other to form a three-dimensional shape that gives them the ability to move and function.
Your hand and wrist are made of:
Bones.
Muscles
Nerves
Tendons
Ligaments
Blood vessels (arteries and veins)
Lymphatic vessels
Hand and wrist bones
Bones provide the main structural support in your hand and wrist. They give them their shape and are the anchors other pieces are connected to.
Hand bones
There are 19 bones in each of your hands. They’re grouped together by their location and function:
Metacarpals: The bones that are in your palm and give it its shape
Phalanges: The individual bones that make up the segments of your fingers and thumb
Sesamoids: Small bones embedded in your tendons that help them move smoothly
Wrist bones
Your wrist is a complex joint made of eight bones that are arranged into two rows.
The proximal row (on the back of your hand, closest to your forearm) includes the:
Scaphoid
Lunate
Triquetrum
Pisiform
The distal row (on the underside of your wrist closest to your palm) includes the:
Trapezium
Trapezoid
Capitate
Hamate
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Your hands and wrists are a complicated network of bones, muscles, nerves, connective tissue and blood vessels. Your hands and wrists help you interact with the world around you every day. Talk to a healthcare provider if you have hand or wrist pain, especially if it’s getting worse over time.
What are the hand and wrist?
Your hand and wrist are complex parts of your body that let you touch and control objects.
They’re a complicated network of bones, muscles, nerves tendons and ligaments, blood vessels and parts of your lymphatic system.
What do the hand and wrist do?
Your hand and wrist help you interact with the world around you. They’re probably the first body part that comes to mind when you think about your sense of touch.
They help you do everything throughout your day that involves touching, holding or using something with your fingers.
Where are the hand and wrist located?
Your wrist is the joint at the end of your forearm. It’s the hinge between your arm and hand that lets you reposition your hand.
Your hand begins where your wrist ends. It includes your palm, fingers and thumb.
How are the hand and wrist structured?
Your hand and wrist are structured to allow you to move, flex and rotate your wrist joint and to use your hand to grab and touch objects.
Your wrist acts like a pivot point that can move in almost any direction as you reach and flex your hand. Think about your hand and wrist like a crane game at an arcade. Your hand is the claw that grabs and holds prizes, and your wrist is the mechanical joint that lets the claw move up and down, and side to side.
Hand and wrist anatomy
The parts that make up your hand and wrist are layered upon each other to form a three-dimensional shape that gives them the ability to move and function.
Your hand and wrist are made of:
Bones.
Muscles
Nerves
Tendons
Ligaments
Blood vessels (arteries and veins)
Lymphatic vessels
Hand and wrist bones
Bones provide the main structural support in your hand and wrist. They give them their shape and are the anchors other pieces are connected to.
Hand bones
There are 19 bones in each of your hands. They’re grouped together by their location and function:
Metacarpals: The bones that are in your palm and give it its shape
Phalanges: The individual bones that make up the segments of your fingers and thumb
Sesamoids: Small bones embedded in your tendons that help them move smoothly
Wrist bones
Your wrist is a complex joint made of eight bones that are arranged into two rows.
The proximal row (on the back of your hand, closest to your forearm) includes the:
Scaphoid
Lunate
Triquetrum
Pisiform
The distal row (on the underside of your wrist closest to your palm) includes the:
Trapezium
Trapezoid
Capitate
Hamate
Your radius (the larger of the two bones in your forearm) forms a joint your scaphoid and lunate bones to form the part of your wrist that helps it move and rotate.
The carpal tunnel is a rounded space between your pisiform, hamate, scaphoid and trapezium. This space is a literal tunnel in your wrist that lets nine tendons, four ligaments and one nerve pass through it to reach the rest of your hand.
Your carpal tunnel is similar to the way that fiber optic cables are buried underground to deliver internet or cable TV service to your home.
Hand and wrist muscles
Muscles are soft tissue made of stretchy fiber. Intrinsic muscles inside your hand work with extrinsic muscles near the outside of your hand and in your forearm to give your hand its strength and dexterity.
Hand muscles
There are 34 muscles in each of your hands. Healthcare providers categorize them into groups, including:
Thenar muscles: Muscles that control your thumb. You can feel them bulge at the base of your thumb in the palm of your hand
Hypothenar muscles: These muscles line the outer edges of your palm on the outside of your pinkie finger. They control the area of your hand that’s opposite your thumb
Interossei muscles: Interossei muscles are between the metacarpal bones in your palm. They help your fingers move side-to-side
Lumbrical muscles: Lumbrical muscles are at the base of your four non-thumb fingers. They help you flex your fingers.
Your muscles and all their possible movements perform two types of grip:
Power: This is where your grip strength comes from. Think about picking up a heavy box or opening a jar
Precision: Precision is using your hand and fingers to move or touch a smaller object. Precision grip uses your fingers’ ability to meet your thumb (sometimes called an opposable grip) to pinch something between them. Picking up a pen off your desk and turning a key in a lock are precision grip motions
Wrist muscles
Your wrist shares muscles with your forearm. Their groups include:
Flexion: Muscles that let you move your wrist down, toward your palm
Extension: Muscles that pull your wrist up, like you would to make a “stop” gesture at someone in front of you
Adduction: Muscles that let you bend your wrist in, toward the center of your body
Abduction: Muscles that let you bend your wrist out, away from the center of your body
Hand nerves and wrist nerves
Nerves control your muscles and help you feel and process sensations, including:
Touch
Temperature
Pain
Pressure
Three main nerves give your hand and wrist sensation:
Radial nerve
Median nerve
Ulnar nerve
All three of these nerves are connected to many branches of smaller nerves that spread out into your hand and wrist.
Hand and wrist tendons
Tendons link your muscles to your bones. They’re like strong, flexible ropes. Your hand and wrist have two groups of tendons:
Extensor tendons: Tendons that help you extend and straighten your fingers, hand and wrist
Flexor tendons: Tendons that help you flex and curl your fingers, hand and wrist
Hand and wrist ligaments
Ligaments are the other type of connective tissue in your hand. If tendons are like ropes, ligaments are more like thick rubber bands. Their main functions include:
Helping your joints move smoothly
Protecting your joints from bending too far
Keeping your joints in the proper alignment
Hand ligaments
There are lots of ligaments in your hand, including:
Collateral ligaments: These ligaments run on the outside edges of your fingers and thumb. They protect your joints from moving too much from side to side
The volar plate: Volar plate ligaments connect your first two finger bones (phalanges) together on each finger. They run under your bones on the palmar side of your hand and keep your fingers from bending too far back when you extend them
Palmar fascia: Your palmar fascia is a thick, triangle-shaped ligament-like structure that runs under the skin of your palm. The narrow point of the triangle is at your wrist, and it gets wider toward the base of your fingers. It helps your hand keep its shape while you move it and prevents your skin from sliding when you’re holding something
Wrist ligaments
Ligaments in your wrist include:
Ulnocarpal and radiocarpal ligaments: Ligaments that stabilize your whole wrist while it moves
Collateral ligaments: These are the same ligaments as the ones in your hand. They run on both sides on the outside of your wrist and hold your wrist in place
Volar carpal ligaments: Ligaments that support and stabilize the bottom (palmar side) of your wrist
Dorsal radiocarpal ligaments: Ligaments that support and stabilize the back side of your wrist
Hand and wrist arteries and blood vessels
Your hand and wrist get blood from two arteries. The radial artery runs along your radius (closer to your thumb). The ulnar artery runs along your ulna (closer to your pinkie finger). These arteries communicate with each other in “arches” that form in your hand. There’s a superficial and deep arch in your hand. Vessels branch off the arches and supply blood to your fingers.
Hand and wrist lymphatics
Your lymphatic system is a network of tissue, vessels and organs that collect excess plasma from your bloodstream and redistribute it throughout your body. Tiny capillaries in your hand capture extra plasma from the blood vessels that supply your hand and wrist. They connect to bigger lymph nodes and vessels in your upper arm.
Conditions and Disorders
What are the common conditions and disorders that affect the wrist and hand?
Many issues can cause hand or wrist pain.
Some of the most common conditions that affect your hand and wrist include:
Carpal tunnel syndrome
Arthritis of the hand or arthritis of the wrist (including rheumatoid arthritis, osteoarthritis and psoriatic arthritis)
Tendinitis
Trigger finger or trigger thumb
Dupuytren contracture
How can I keep my hand and wrist healthy?
One of the best ways to keep your hand and wrist healthy is to avoid overusing them. Any activity or job that makes you use them repeatedly can lead to a repetitive strain injury.
During sports or other physical activities:
Wear the right protective equipment
Don’t “play through it” if you feel pain during or after physical activity
Give your body time to rest and recover after intense activity
Stretch and warm up before playing sports or working out
Cool down and stretch after physical activity
Avoid extending or flexing your hands and wrists too far
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Physical therapy is vital for PCL injury recovery. Key stages include:
Acute Phase (First 72 Hours):
Rest and reduced load on the injured knee.
Ice application to reduce swelling and pain.
Elevation of the leg to improve circulation.
Early Recovery Phase:
Gentle exercises to improve mobility.
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Physical therapy is vital for PCL injury recovery. Key stages include:
Acute Phase (First 72 Hours):
Rest and reduced load on the injured knee.
Ice application to reduce swelling and pain.
Elevation of the leg to improve circulation.
Early Recovery Phase:
Gentle exercises to improve mobility.
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Physical therapy is vital for PCL injury recovery. Key stages include:
Acute Phase (First 72 Hours):
Rest and reduced load on the injured knee.
Ice application to reduce swelling and pain.
Elevation of the leg to improve circulation.
Early Recovery Phase:
Gentle exercises to improve mobility.
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Diagnosis is conducted through physical examination, MRI, and X-rays.
Physical Therapy for Recovery
Physical therapy is vital for PCL injury recovery. Key stages include:
Acute Phase (First 72 Hours):
Rest and reduced load on the injured knee.
Ice application to reduce swelling and pain.
Elevation of the leg to improve circulation.
Early Recovery Phase:
Gentle exercises to improve mobility.
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Diagnosis is conducted through physical examination, MRI, and X-rays.
Physical Therapy for Recovery
Physical therapy is vital for PCL injury recovery. Key stages include:
Acute Phase (First 72 Hours):
Rest and reduced load on the injured knee.
Ice application to reduce swelling and pain.
Elevation of the leg to improve circulation.
Early Recovery Phase:
Gentle exercises to improve mobility.
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Diagnosis is conducted through physical examination, MRI, and X-rays.
Physical Therapy for Recovery
Physical therapy is vital for PCL injury recovery. Key stages include:
Acute Phase (First 72 Hours):
Rest and reduced load on the injured knee.
Ice application to reduce swelling and pain.
Elevation of the leg to improve circulation.
Early Recovery Phase:
Gentle exercises to improve mobility.
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Diagnosis is conducted through physical examination, MRI, and X-rays.
Physical Therapy for Recovery
Physical therapy is vital for PCL injury recovery. Key stages include:
Acute Phase (First 72 Hours):
Rest and reduced load on the injured knee.
Ice application to reduce swelling and pain.
Elevation of the leg to improve circulation.
Early Recovery Phase:
Gentle exercises to improve mobility.
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Diagnosis is conducted through physical examination, MRI, and X-rays.
Physical Therapy for Recovery
Physical therapy is vital for PCL injury recovery. Key stages include:
Acute Phase (First 72 Hours):
Rest and reduced load on the injured knee.
Ice application to reduce swelling and pain.
Elevation of the leg to improve circulation.
Early Recovery Phase:
Gentle exercises to improve mobility.
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Posterior Cruciate Ligaments of the Knee: Injuries and Physical Therapy for Recovery
About
The posterior cruciate ligaments (PCL) play a crucial role in stabilizing the knee joint by preventing the tibia from moving too far backward relative to the femur. Injuries to the PCL are common among athletes and can significantly impact mobility.
Causes of PCL Injuries
PCL injuries typically occur due to:
Car accidents.
Sports injuries (e.g., football, basketball).
Falls on a bent knee.
Symptoms and Diagnosis
Symptoms of PCL injury include:
Acute pain and swelling.
Knee instability.
Limited range of motion.
Diagnosis is conducted through physical examination, MRI, and X-rays.
Physical Therapy for Recovery
Physical therapy is vital for PCL injury recovery. Key stages include:
Acute Phase (First 72 Hours):
Rest and reduced load on the injured knee.
Ice application to reduce swelling and pain.
Elevation of the leg to improve circulation.
Early Recovery Phase:
Gentle exercises to improve mobility.
Passive and active exercises to strengthen muscles around the knee.
Middle Recovery Phase:
Exercises to enhance coordination and balance.
Stretching and strengthening exercises.
Late Recovery Phase:
Intensive exercises to restore strength and endurance.
Gradual return to sports training under the supervision of a physiotherapist.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
2. Stretching and Strengthening Exercises: Specific exercises to stretch and strengthen the muscles of the back and shoulders can help prevent recurrence. Examples include pectoral stretches, the “cat-cow” exercise, and exercises with resistance bands.
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
2. Stretching and Strengthening Exercises: Specific exercises to stretch and strengthen the muscles of the back and shoulders can help prevent recurrence. Examples include pectoral stretches, the “cat-cow” exercise, and exercises with resistance bands.
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
2. Stretching and Strengthening Exercises: Specific exercises to stretch and strengthen the muscles of the back and shoulders can help prevent recurrence. Examples include pectoral stretches, the “cat-cow” exercise, and exercises with resistance bands.
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
1. Physical Therapy: Regular physical therapy sessions can help relieve tension and improve mobility. Key methods include massage, stretching exercises, and manual therapy.
2. Stretching and Strengthening Exercises: Specific exercises to stretch and strengthen the muscles of the back and shoulders can help prevent recurrence. Examples include pectoral stretches, the “cat-cow” exercise, and exercises with resistance bands.
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
1. Physical Therapy: Regular physical therapy sessions can help relieve tension and improve mobility. Key methods include massage, stretching exercises, and manual therapy.
2. Stretching and Strengthening Exercises: Specific exercises to stretch and strengthen the muscles of the back and shoulders can help prevent recurrence. Examples include pectoral stretches, the “cat-cow” exercise, and exercises with resistance bands.
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
1. Physical Therapy: Regular physical therapy sessions can help relieve tension and improve mobility. Key methods include massage, stretching exercises, and manual therapy.
2. Stretching and Strengthening Exercises: Specific exercises to stretch and strengthen the muscles of the back and shoulders can help prevent recurrence. Examples include pectoral stretches, the “cat-cow” exercise, and exercises with resistance bands.
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
3. Spasms and Stiffness: A feeling of stiffness and spasms in the shoulder blade area.
Treatment and Prevention Methods
1. Physical Therapy: Regular physical therapy sessions can help relieve tension and improve mobility. Key methods include massage, stretching exercises, and manual therapy.
2. Stretching and Strengthening Exercises: Specific exercises to stretch and strengthen the muscles of the back and shoulders can help prevent recurrence. Examples include pectoral stretches, the “cat-cow” exercise, and exercises with resistance bands.
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
2. Limited Mobility: Difficulty in lifting the arm or performing certain movements.
3. Spasms and Stiffness: A feeling of stiffness and spasms in the shoulder blade area.
Treatment and Prevention Methods
1. Physical Therapy: Regular physical therapy sessions can help relieve tension and improve mobility. Key methods include massage, stretching exercises, and manual therapy.
2. Stretching and Strengthening Exercises: Specific exercises to stretch and strengthen the muscles of the back and shoulders can help prevent recurrence. Examples include pectoral stretches, the “cat-cow” exercise, and exercises with resistance bands.
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
1. Pain Under the Shoulder Blade: Sharp or dull pain that worsens with movement of the arm or shoulder blade.
2. Limited Mobility: Difficulty in lifting the arm or performing certain movements.
3. Spasms and Stiffness: A feeling of stiffness and spasms in the shoulder blade area.
Treatment and Prevention Methods
1. Physical Therapy: Regular physical therapy sessions can help relieve tension and improve mobility. Key methods include massage, stretching exercises, and manual therapy.
2. Stretching and Strengthening Exercises: Specific exercises to stretch and strengthen the muscles of the back and shoulders can help prevent recurrence. Examples include pectoral stretches, the “cat-cow” exercise, and exercises with resistance bands.
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
4. Insufficient Recovery: Lack of adequate recovery time between workouts can contribute to the buildup of muscle tension.
Symptoms
1. Pain Under the Shoulder Blade: Sharp or dull pain that worsens with movement of the arm or shoulder blade.
2. Limited Mobility: Difficulty in lifting the arm or performing certain movements.
3. Spasms and Stiffness: A feeling of stiffness and spasms in the shoulder blade area.
Treatment and Prevention Methods
1. Physical Therapy: Regular physical therapy sessions can help relieve tension and improve mobility. Key methods include massage, stretching exercises, and manual therapy.
2. Stretching and Strengthening Exercises: Specific exercises to stretch and strengthen the muscles of the back and shoulders can help prevent recurrence. Examples include pectoral stretches, the “cat-cow” exercise, and exercises with resistance bands.
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
3. Injuries: Bruises, strains, and other injuries can cause muscle spasms and tightness. This is particularly relevant for contact sports like wrestling or football.
4. Insufficient Recovery: Lack of adequate recovery time between workouts can contribute to the buildup of muscle tension.
Symptoms
1. Pain Under the Shoulder Blade: Sharp or dull pain that worsens with movement of the arm or shoulder blade.
2. Limited Mobility: Difficulty in lifting the arm or performing certain movements.
3. Spasms and Stiffness: A feeling of stiffness and spasms in the shoulder blade area.
Treatment and Prevention Methods
1. Physical Therapy: Regular physical therapy sessions can help relieve tension and improve mobility. Key methods include massage, stretching exercises, and manual therapy.
2. Stretching and Strengthening Exercises: Specific exercises to stretch and strengthen the muscles of the back and shoulders can help prevent recurrence. Examples include pectoral stretches, the “cat-cow” exercise, and exercises with resistance bands.
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
2. Poor Posture: Maintaining an improper posture for extended periods, especially during exercises or in daily life, can lead to muscle tightness under the shoulder blade.
3. Injuries: Bruises, strains, and other injuries can cause muscle spasms and tightness. This is particularly relevant for contact sports like wrestling or football.
4. Insufficient Recovery: Lack of adequate recovery time between workouts can contribute to the buildup of muscle tension.
Symptoms
1. Pain Under the Shoulder Blade: Sharp or dull pain that worsens with movement of the arm or shoulder blade.
2. Limited Mobility: Difficulty in lifting the arm or performing certain movements.
3. Spasms and Stiffness: A feeling of stiffness and spasms in the shoulder blade area.
Treatment and Prevention Methods
1. Physical Therapy: Regular physical therapy sessions can help relieve tension and improve mobility. Key methods include massage, stretching exercises, and manual therapy.
2. Stretching and Strengthening Exercises: Specific exercises to stretch and strengthen the muscles of the back and shoulders can help prevent recurrence. Examples include pectoral stretches, the “cat-cow” exercise, and exercises with resistance bands.
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Causes of Muscle Tightness Under the Shoulder Blade
1. Muscle Overuse: Continuous intense training can lead to muscle overuse and spasms. This is often seen in swimmers, tennis players, and throwers, whose muscles are constantly subjected to high loads.
2. Poor Posture: Maintaining an improper posture for extended periods, especially during exercises or in daily life, can lead to muscle tightness under the shoulder blade.
3. Injuries: Bruises, strains, and other injuries can cause muscle spasms and tightness. This is particularly relevant for contact sports like wrestling or football.
4. Insufficient Recovery: Lack of adequate recovery time between workouts can contribute to the buildup of muscle tension.
Symptoms
1. Pain Under the Shoulder Blade: Sharp or dull pain that worsens with movement of the arm or shoulder blade.
2. Limited Mobility: Difficulty in lifting the arm or performing certain movements.
3. Spasms and Stiffness: A feeling of stiffness and spasms in the shoulder blade area.
Treatment and Prevention Methods
1. Physical Therapy: Regular physical therapy sessions can help relieve tension and improve mobility. Key methods include massage, stretching exercises, and manual therapy.
2. Stretching and Strengthening Exercises: Specific exercises to stretch and strengthen the muscles of the back and shoulders can help prevent recurrence. Examples include pectoral stretches, the “cat-cow” exercise, and exercises with resistance bands.
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Muscle Tightness Under the Shoulder Blade in Athletes: Causes, Symptoms, and Treatment Methods
Introduction
Muscle tightness under the shoulder blade is a common issue among athletes, especially those involved in sports that place a high demand on the upper body. This condition can cause significant discomfort and restrict movement, negatively affecting athletic performance.
Causes of Muscle Tightness Under the Shoulder Blade
1. Muscle Overuse: Continuous intense training can lead to muscle overuse and spasms. This is often seen in swimmers, tennis players, and throwers, whose muscles are constantly subjected to high loads.
2. Poor Posture: Maintaining an improper posture for extended periods, especially during exercises or in daily life, can lead to muscle tightness under the shoulder blade.
3. Injuries: Bruises, strains, and other injuries can cause muscle spasms and tightness. This is particularly relevant for contact sports like wrestling or football.
4. Insufficient Recovery: Lack of adequate recovery time between workouts can contribute to the buildup of muscle tension.
Symptoms
1. Pain Under the Shoulder Blade: Sharp or dull pain that worsens with movement of the arm or shoulder blade.
2. Limited Mobility: Difficulty in lifting the arm or performing certain movements.
3. Spasms and Stiffness: A feeling of stiffness and spasms in the shoulder blade area.
Treatment and Prevention Methods
1. Physical Therapy: Regular physical therapy sessions can help relieve tension and improve mobility. Key methods include massage, stretching exercises, and manual therapy.
2. Stretching and Strengthening Exercises: Specific exercises to stretch and strengthen the muscles of the back and shoulders can help prevent recurrence. Examples include pectoral stretches, the “cat-cow” exercise, and exercises with resistance bands.
3. Proper Posture: Maintaining proper posture both during workouts and in daily life is crucial. Using ergonomic chairs and taking regular breaks to stretch can help prevent muscle tightness.
4. Ice and Heat: For acute pain, ice can be used to reduce inflammation, followed by heat to relax the muscles.
5. Medication: In some cases, pain relievers and anti-inflammatory drugs prescribed by a doctor can be helpful.
Conclusion
Muscle tightness under the shoulder blade is a problem many athletes face. However, with timely and proper treatment and prevention, the risk of this issue can be significantly reduced, and the quality of training and athletic performance can be improved. It is important to seek help from professionals such as physical therapists to receive professional assistance and recommendations.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Conclusion
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Conclusion
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Each injury is unique, and the recovery process requires an individual approach. Physical therapists assess the patient’s condition, consider their physical activity, age, injury level, and develop personalized rehabilitation programs. This approach allows achieving the best results in the shortest time.
Education and Prevention
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Conclusion
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Each injury is unique, and the recovery process requires an individual approach. Physical therapists assess the patient’s condition, consider their physical activity, age, injury level, and develop personalized rehabilitation programs. This approach allows achieving the best results in the shortest time.
Education and Prevention
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Conclusion
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Each injury is unique, and the recovery process requires an individual approach. Physical therapists assess the patient’s condition, consider their physical activity, age, injury level, and develop personalized rehabilitation programs. This approach allows achieving the best results in the shortest time.
Education and Prevention
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Conclusion
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Injuries can affect coordination and balance, which is especially important for athletes. Physical therapists conduct special training to restore these skills, helping patients return to normal life and sports activities faster.
Individual Approach
Each injury is unique, and the recovery process requires an individual approach. Physical therapists assess the patient’s condition, consider their physical activity, age, injury level, and develop personalized rehabilitation programs. This approach allows achieving the best results in the shortest time.
Education and Prevention
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Conclusion
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Injuries can affect coordination and balance, which is especially important for athletes. Physical therapists conduct special training to restore these skills, helping patients return to normal life and sports activities faster.
Individual Approach
Each injury is unique, and the recovery process requires an individual approach. Physical therapists assess the patient’s condition, consider their physical activity, age, injury level, and develop personalized rehabilitation programs. This approach allows achieving the best results in the shortest time.
Education and Prevention
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Conclusion
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Injuries can affect coordination and balance, which is especially important for athletes. Physical therapists conduct special training to restore these skills, helping patients return to normal life and sports activities faster.
Individual Approach
Each injury is unique, and the recovery process requires an individual approach. Physical therapists assess the patient’s condition, consider their physical activity, age, injury level, and develop personalized rehabilitation programs. This approach allows achieving the best results in the shortest time.
Education and Prevention
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Conclusion
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Muscle weakness is another common problem after injuries. Physical therapists use various methods, including strength exercises, to restore and strengthen muscle mass. Strong muscles provide better support for the joints and help avoid recurrent injuries.
Coordination and Balance
Injuries can affect coordination and balance, which is especially important for athletes. Physical therapists conduct special training to restore these skills, helping patients return to normal life and sports activities faster.
Individual Approach
Each injury is unique, and the recovery process requires an individual approach. Physical therapists assess the patient’s condition, consider their physical activity, age, injury level, and develop personalized rehabilitation programs. This approach allows achieving the best results in the shortest time.
Education and Prevention
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Conclusion
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
After an injury, there is often a restriction of mobility and flexibility in the joints and muscles. Physical therapists develop individual exercise programs aimed at restoring the mobility and flexibility of the affected areas. Regular performance of such exercises helps prevent the formation of scars and contractures, improving the overall condition of the patient.
Strengthening Muscles
Muscle weakness is another common problem after injuries. Physical therapists use various methods, including strength exercises, to restore and strengthen muscle mass. Strong muscles provide better support for the joints and help avoid recurrent injuries.
Coordination and Balance
Injuries can affect coordination and balance, which is especially important for athletes. Physical therapists conduct special training to restore these skills, helping patients return to normal life and sports activities faster.
Individual Approach
Each injury is unique, and the recovery process requires an individual approach. Physical therapists assess the patient’s condition, consider their physical activity, age, injury level, and develop personalized rehabilitation programs. This approach allows achieving the best results in the shortest time.
Education and Prevention
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Conclusion
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Good blood circulation is necessary to deliver oxygen and nutrients to damaged tissues, which accelerates their healing process. Physical therapy includes exercises and massage that help improve blood circulation in the affected area. This contributes to faster tissue healing and reduces swelling.
Restoring Mobility and Flexibility
After an injury, there is often a restriction of mobility and flexibility in the joints and muscles. Physical therapists develop individual exercise programs aimed at restoring the mobility and flexibility of the affected areas. Regular performance of such exercises helps prevent the formation of scars and contractures, improving the overall condition of the patient.
Strengthening Muscles
Muscle weakness is another common problem after injuries. Physical therapists use various methods, including strength exercises, to restore and strengthen muscle mass. Strong muscles provide better support for the joints and help avoid recurrent injuries.
Coordination and Balance
Injuries can affect coordination and balance, which is especially important for athletes. Physical therapists conduct special training to restore these skills, helping patients return to normal life and sports activities faster.
Individual Approach
Each injury is unique, and the recovery process requires an individual approach. Physical therapists assess the patient’s condition, consider their physical activity, age, injury level, and develop personalized rehabilitation programs. This approach allows achieving the best results in the shortest time.
Education and Prevention
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Conclusion
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
One of the first stages of recovery after an injury is reducing pain and inflammation. Physical therapists use various methods, such as cold compresses, ultrasound therapy, and electrical stimulation, to help reduce inflammation and pain. These methods not only ease discomfort but also create conditions for further effective treatment.
Improving Blood Circulation
Good blood circulation is necessary to deliver oxygen and nutrients to damaged tissues, which accelerates their healing process. Physical therapy includes exercises and massage that help improve blood circulation in the affected area. This contributes to faster tissue healing and reduces swelling.
Restoring Mobility and Flexibility
After an injury, there is often a restriction of mobility and flexibility in the joints and muscles. Physical therapists develop individual exercise programs aimed at restoring the mobility and flexibility of the affected areas. Regular performance of such exercises helps prevent the formation of scars and contractures, improving the overall condition of the patient.
Strengthening Muscles
Muscle weakness is another common problem after injuries. Physical therapists use various methods, including strength exercises, to restore and strengthen muscle mass. Strong muscles provide better support for the joints and help avoid recurrent injuries.
Coordination and Balance
Injuries can affect coordination and balance, which is especially important for athletes. Physical therapists conduct special training to restore these skills, helping patients return to normal life and sports activities faster.
Individual Approach
Each injury is unique, and the recovery process requires an individual approach. Physical therapists assess the patient’s condition, consider their physical activity, age, injury level, and develop personalized rehabilitation programs. This approach allows achieving the best results in the shortest time.
Education and Prevention
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Conclusion
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
How Physical Therapy Helps Speed Up Recovery After Injuries
Injuries are an integral part of the lives of many people, especially athletes. Regardless of how experienced and careful you are, injuries can happen at any moment. It is important not only to properly treat the injury but also to speed up the recovery process to return to an active lifestyle faster. Physical therapy plays a key role in this process. Let’s look at how exactly physical therapy helps speed up recovery after injuries.
Pain Relief and Inflammation Reduction
One of the first stages of recovery after an injury is reducing pain and inflammation. Physical therapists use various methods, such as cold compresses, ultrasound therapy, and electrical stimulation, to help reduce inflammation and pain. These methods not only ease discomfort but also create conditions for further effective treatment.
Improving Blood Circulation
Good blood circulation is necessary to deliver oxygen and nutrients to damaged tissues, which accelerates their healing process. Physical therapy includes exercises and massage that help improve blood circulation in the affected area. This contributes to faster tissue healing and reduces swelling.
Restoring Mobility and Flexibility
After an injury, there is often a restriction of mobility and flexibility in the joints and muscles. Physical therapists develop individual exercise programs aimed at restoring the mobility and flexibility of the affected areas. Regular performance of such exercises helps prevent the formation of scars and contractures, improving the overall condition of the patient.
Strengthening Muscles
Muscle weakness is another common problem after injuries. Physical therapists use various methods, including strength exercises, to restore and strengthen muscle mass. Strong muscles provide better support for the joints and help avoid recurrent injuries.
Coordination and Balance
Injuries can affect coordination and balance, which is especially important for athletes. Physical therapists conduct special training to restore these skills, helping patients return to normal life and sports activities faster.
Individual Approach
Each injury is unique, and the recovery process requires an individual approach. Physical therapists assess the patient’s condition, consider their physical activity, age, injury level, and develop personalized rehabilitation programs. This approach allows achieving the best results in the shortest time.
Education and Prevention
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Conclusion
Physical therapy not only treats injuries but also teaches patients how to avoid recurrent injuries. Physical therapists provide recommendations on the correct exercise techniques, explain the importance of warm-up and cool-down, and share tips on maintaining a healthy lifestyle.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Walking. Sciatica often causes visible changes in how you walk. Your provider will watch for those changes as part of diagnosing sciatica.
Straight leg raise test. This involves having you lie on an exam table with your legs straight out. They’ll slowly raise your legs one at a time toward the ceiling and ask when you start to feel pain or other symptoms. These can help pinpoint the cause of sciatica and how to manage it.
Other flexibility and strength checks. These can help your provider determine if any other factors are causing or contributing to your sciatica.
What tests will be done to diagnose this condition?
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
A healthcare provider can diagnose sciatica using a combination of methods. They’ll review your medical history and ask about your symptoms. They’ll also do a physical examination. That exam will include:
Walking. Sciatica often causes visible changes in how you walk. Your provider will watch for those changes as part of diagnosing sciatica.
Straight leg raise test. This involves having you lie on an exam table with your legs straight out. They’ll slowly raise your legs one at a time toward the ceiling and ask when you start to feel pain or other symptoms. These can help pinpoint the cause of sciatica and how to manage it.
Other flexibility and strength checks. These can help your provider determine if any other factors are causing or contributing to your sciatica.
What tests will be done to diagnose this condition?
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
A healthcare provider can diagnose sciatica using a combination of methods. They’ll review your medical history and ask about your symptoms. They’ll also do a physical examination. That exam will include:
Walking. Sciatica often causes visible changes in how you walk. Your provider will watch for those changes as part of diagnosing sciatica.
Straight leg raise test. This involves having you lie on an exam table with your legs straight out. They’ll slowly raise your legs one at a time toward the ceiling and ask when you start to feel pain or other symptoms. These can help pinpoint the cause of sciatica and how to manage it.
Other flexibility and strength checks. These can help your provider determine if any other factors are causing or contributing to your sciatica.
What tests will be done to diagnose this condition?
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
A healthcare provider can diagnose sciatica using a combination of methods. They’ll review your medical history and ask about your symptoms. They’ll also do a physical examination. That exam will include:
Walking. Sciatica often causes visible changes in how you walk. Your provider will watch for those changes as part of diagnosing sciatica.
Straight leg raise test. This involves having you lie on an exam table with your legs straight out. They’ll slowly raise your legs one at a time toward the ceiling and ask when you start to feel pain or other symptoms. These can help pinpoint the cause of sciatica and how to manage it.
Other flexibility and strength checks. These can help your provider determine if any other factors are causing or contributing to your sciatica.
What tests will be done to diagnose this condition?
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
A healthcare provider can diagnose sciatica using a combination of methods. They’ll review your medical history and ask about your symptoms. They’ll also do a physical examination. That exam will include:
Walking. Sciatica often causes visible changes in how you walk. Your provider will watch for those changes as part of diagnosing sciatica.
Straight leg raise test. This involves having you lie on an exam table with your legs straight out. They’ll slowly raise your legs one at a time toward the ceiling and ask when you start to feel pain or other symptoms. These can help pinpoint the cause of sciatica and how to manage it.
Other flexibility and strength checks. These can help your provider determine if any other factors are causing or contributing to your sciatica.
What tests will be done to diagnose this condition?
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Having a current or previous injury. An injury to your spine or lower back increases your risk of developing sciatica.
Normal wear-and-tear. As you get older, normal wear-and-tear on your spine can lead to pinched nerves, herniated disks and other conditions that can cause sciatica. Age-related conditions like osteoarthritis can also play a role.
Having excess weight or obesity. Your spine is like a construction crane when you stand upright. The weight you carry in the front of your body is what your spine (crane) has to hoist. Muscles in your back are like the winch and cable, pulling to keep you vertical. The more weight you have, the more your back muscles have to work. That can lead to back strains, pain and other issues.
Having insufficient core strength. Your “core” is the term for the muscles of your back and abdomen (stomach area). Like in the crane analogy, having a stronger core is like upgrading the crane’s components to handle a heavier load. The muscles of your abdomen are important because they help anchor your back muscles.
Your job. Jobs that require heavy lifting, a lot of bending, or working in awkward or unusual positions may increase your risk of low back problems. However, jobs with prolonged sitting — especially without proper back support — may also increase your risk of low back problems.
Not using good posture and form when lifting. Even if you’re physically fit and active, you can still be prone to sciatica if you don’t follow proper body form during weight lifting, strength training or similar activities.
Having diabetes. Type 2 diabetes increases your risk of diabetes-related peripheral neuropathy. That damages your nerves, including any of the nerves that can cause or contribute to sciatica.
Physical inactivity. Sitting for long periods and a lack of physical activity can contribute to an increased risk of sciatica.
Using tobacco. Nicotine use can affect circulation and increase your risk of chronic pain. That includes conditions like sciatica.
Unknown causes. Many cases of sciatica don’t have a cause that healthcare providers can find.
What are the complications of sciatica?
Most people recover fully from sciatica. However, a possible complication of sciatica is chronic (long-term) pain.
If there’s serious damage to an affected nerve, chronic muscle weakness, such as a “drop foot,” might happen. That’s when nerve damage causes numbness in your foot, which makes normal walking difficult or even impossible.
Sciatica can also potentially cause permanent nerve damage, resulting in a loss of feeling in the affected legs.
Diagnosis and Tests
How is sciatica diagnosed?
A healthcare provider can diagnose sciatica using a combination of methods. They’ll review your medical history and ask about your symptoms. They’ll also do a physical examination. That exam will include:
Walking. Sciatica often causes visible changes in how you walk. Your provider will watch for those changes as part of diagnosing sciatica.
Straight leg raise test. This involves having you lie on an exam table with your legs straight out. They’ll slowly raise your legs one at a time toward the ceiling and ask when you start to feel pain or other symptoms. These can help pinpoint the cause of sciatica and how to manage it.
Other flexibility and strength checks. These can help your provider determine if any other factors are causing or contributing to your sciatica.
What tests will be done to diagnose this condition?
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Because sciatica can happen for so many reasons, there are many potential risk factors, which include, but aren’t limited to:
Having a current or previous injury. An injury to your spine or lower back increases your risk of developing sciatica.
Normal wear-and-tear. As you get older, normal wear-and-tear on your spine can lead to pinched nerves, herniated disks and other conditions that can cause sciatica. Age-related conditions like osteoarthritis can also play a role.
Having excess weight or obesity. Your spine is like a construction crane when you stand upright. The weight you carry in the front of your body is what your spine (crane) has to hoist. Muscles in your back are like the winch and cable, pulling to keep you vertical. The more weight you have, the more your back muscles have to work. That can lead to back strains, pain and other issues.
Having insufficient core strength. Your “core” is the term for the muscles of your back and abdomen (stomach area). Like in the crane analogy, having a stronger core is like upgrading the crane’s components to handle a heavier load. The muscles of your abdomen are important because they help anchor your back muscles.
Your job. Jobs that require heavy lifting, a lot of bending, or working in awkward or unusual positions may increase your risk of low back problems. However, jobs with prolonged sitting — especially without proper back support — may also increase your risk of low back problems.
Not using good posture and form when lifting. Even if you’re physically fit and active, you can still be prone to sciatica if you don’t follow proper body form during weight lifting, strength training or similar activities.
Having diabetes. Type 2 diabetes increases your risk of diabetes-related peripheral neuropathy. That damages your nerves, including any of the nerves that can cause or contribute to sciatica.
Physical inactivity. Sitting for long periods and a lack of physical activity can contribute to an increased risk of sciatica.
Using tobacco. Nicotine use can affect circulation and increase your risk of chronic pain. That includes conditions like sciatica.
Unknown causes. Many cases of sciatica don’t have a cause that healthcare providers can find.
What are the complications of sciatica?
Most people recover fully from sciatica. However, a possible complication of sciatica is chronic (long-term) pain.
If there’s serious damage to an affected nerve, chronic muscle weakness, such as a “drop foot,” might happen. That’s when nerve damage causes numbness in your foot, which makes normal walking difficult or even impossible.
Sciatica can also potentially cause permanent nerve damage, resulting in a loss of feeling in the affected legs.
Diagnosis and Tests
How is sciatica diagnosed?
A healthcare provider can diagnose sciatica using a combination of methods. They’ll review your medical history and ask about your symptoms. They’ll also do a physical examination. That exam will include:
Walking. Sciatica often causes visible changes in how you walk. Your provider will watch for those changes as part of diagnosing sciatica.
Straight leg raise test. This involves having you lie on an exam table with your legs straight out. They’ll slowly raise your legs one at a time toward the ceiling and ask when you start to feel pain or other symptoms. These can help pinpoint the cause of sciatica and how to manage it.
Other flexibility and strength checks. These can help your provider determine if any other factors are causing or contributing to your sciatica.
What tests will be done to diagnose this condition?
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Pain. Sciatica pain happens because of pressure on the affected nerve(s). Most people describe sciatica pain as burning or like an electric shock. This pain also often shoots or radiates down the leg on the affected side. Pain commonly happens with coughing, sneezing, bending or lifting your legs upward when lying on your back.
Tingling or “pins and needles” (paresthesia). This is similar to the feeling you have when a leg falls asleep because you sat cross-legged.
Numbness. This is when you can’t feel sensations on the skin in the affected areas of your back or leg. It happens because signals from your back or leg are having trouble reaching your brain.
Muscle weakness. This is a more severe symptom. It means that muscle command signals are having trouble reaching their destinations in your back or legs.
Urinary incontinence or fecal incontinence. This is a very severe symptom. It means signals that control your bladder and bowels aren’t reaching their destinations.
What causes sciatica?
Sciatica can happen because of any condition that affects the sciatic nerve. It can also happen because of conditions affecting any of the five spinal nerves that bundle to form the sciatic nerve.
Conditions that can cause sciatica include:
Herniated disks.
Degenerative disk disease.
Spinal stenosis.
Foraminal stenosis.
Spondylolisthesis.
Osteoarthritis.
Injuries.
Pregnancy.
Tumors, cysts or other growths.
Conus medullas syndrome.
Cauda equina syndrome.
What are the risk factors for sciatica?
Because sciatica can happen for so many reasons, there are many potential risk factors, which include, but aren’t limited to:
Having a current or previous injury. An injury to your spine or lower back increases your risk of developing sciatica.
Normal wear-and-tear. As you get older, normal wear-and-tear on your spine can lead to pinched nerves, herniated disks and other conditions that can cause sciatica. Age-related conditions like osteoarthritis can also play a role.
Having excess weight or obesity. Your spine is like a construction crane when you stand upright. The weight you carry in the front of your body is what your spine (crane) has to hoist. Muscles in your back are like the winch and cable, pulling to keep you vertical. The more weight you have, the more your back muscles have to work. That can lead to back strains, pain and other issues.
Having insufficient core strength. Your “core” is the term for the muscles of your back and abdomen (stomach area). Like in the crane analogy, having a stronger core is like upgrading the crane’s components to handle a heavier load. The muscles of your abdomen are important because they help anchor your back muscles.
Your job. Jobs that require heavy lifting, a lot of bending, or working in awkward or unusual positions may increase your risk of low back problems. However, jobs with prolonged sitting — especially without proper back support — may also increase your risk of low back problems.
Not using good posture and form when lifting. Even if you’re physically fit and active, you can still be prone to sciatica if you don’t follow proper body form during weight lifting, strength training or similar activities.
Having diabetes. Type 2 diabetes increases your risk of diabetes-related peripheral neuropathy. That damages your nerves, including any of the nerves that can cause or contribute to sciatica.
Physical inactivity. Sitting for long periods and a lack of physical activity can contribute to an increased risk of sciatica.
Using tobacco. Nicotine use can affect circulation and increase your risk of chronic pain. That includes conditions like sciatica.
Unknown causes. Many cases of sciatica don’t have a cause that healthcare providers can find.
What are the complications of sciatica?
Most people recover fully from sciatica. However, a possible complication of sciatica is chronic (long-term) pain.
If there’s serious damage to an affected nerve, chronic muscle weakness, such as a “drop foot,” might happen. That’s when nerve damage causes numbness in your foot, which makes normal walking difficult or even impossible.
Sciatica can also potentially cause permanent nerve damage, resulting in a loss of feeling in the affected legs.
Diagnosis and Tests
How is sciatica diagnosed?
A healthcare provider can diagnose sciatica using a combination of methods. They’ll review your medical history and ask about your symptoms. They’ll also do a physical examination. That exam will include:
Walking. Sciatica often causes visible changes in how you walk. Your provider will watch for those changes as part of diagnosing sciatica.
Straight leg raise test. This involves having you lie on an exam table with your legs straight out. They’ll slowly raise your legs one at a time toward the ceiling and ask when you start to feel pain or other symptoms. These can help pinpoint the cause of sciatica and how to manage it.
Other flexibility and strength checks. These can help your provider determine if any other factors are causing or contributing to your sciatica.
What tests will be done to diagnose this condition?
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Pain. Sciatica pain happens because of pressure on the affected nerve(s). Most people describe sciatica pain as burning or like an electric shock. This pain also often shoots or radiates down the leg on the affected side. Pain commonly happens with coughing, sneezing, bending or lifting your legs upward when lying on your back.
Tingling or “pins and needles” (paresthesia). This is similar to the feeling you have when a leg falls asleep because you sat cross-legged.
Numbness. This is when you can’t feel sensations on the skin in the affected areas of your back or leg. It happens because signals from your back or leg are having trouble reaching your brain.
Muscle weakness. This is a more severe symptom. It means that muscle command signals are having trouble reaching their destinations in your back or legs.
Urinary incontinence or fecal incontinence. This is a very severe symptom. It means signals that control your bladder and bowels aren’t reaching their destinations.
What causes sciatica?
Sciatica can happen because of any condition that affects the sciatic nerve. It can also happen because of conditions affecting any of the five spinal nerves that bundle to form the sciatic nerve.
Conditions that can cause sciatica include:
Herniated disks.
Degenerative disk disease.
Spinal stenosis.
Foraminal stenosis.
Spondylolisthesis.
Osteoarthritis.
Injuries.
Pregnancy.
Tumors, cysts or other growths.
Conus medullas syndrome.
Cauda equina syndrome.
What are the risk factors for sciatica?
Because sciatica can happen for so many reasons, there are many potential risk factors, which include, but aren’t limited to:
Having a current or previous injury. An injury to your spine or lower back increases your risk of developing sciatica.
Normal wear-and-tear. As you get older, normal wear-and-tear on your spine can lead to pinched nerves, herniated disks and other conditions that can cause sciatica. Age-related conditions like osteoarthritis can also play a role.
Having excess weight or obesity. Your spine is like a construction crane when you stand upright. The weight you carry in the front of your body is what your spine (crane) has to hoist. Muscles in your back are like the winch and cable, pulling to keep you vertical. The more weight you have, the more your back muscles have to work. That can lead to back strains, pain and other issues.
Having insufficient core strength. Your “core” is the term for the muscles of your back and abdomen (stomach area). Like in the crane analogy, having a stronger core is like upgrading the crane’s components to handle a heavier load. The muscles of your abdomen are important because they help anchor your back muscles.
Your job. Jobs that require heavy lifting, a lot of bending, or working in awkward or unusual positions may increase your risk of low back problems. However, jobs with prolonged sitting — especially without proper back support — may also increase your risk of low back problems.
Not using good posture and form when lifting. Even if you’re physically fit and active, you can still be prone to sciatica if you don’t follow proper body form during weight lifting, strength training or similar activities.
Having diabetes. Type 2 diabetes increases your risk of diabetes-related peripheral neuropathy. That damages your nerves, including any of the nerves that can cause or contribute to sciatica.
Physical inactivity. Sitting for long periods and a lack of physical activity can contribute to an increased risk of sciatica.
Using tobacco. Nicotine use can affect circulation and increase your risk of chronic pain. That includes conditions like sciatica.
Unknown causes. Many cases of sciatica don’t have a cause that healthcare providers can find.
What are the complications of sciatica?
Most people recover fully from sciatica. However, a possible complication of sciatica is chronic (long-term) pain.
If there’s serious damage to an affected nerve, chronic muscle weakness, such as a “drop foot,” might happen. That’s when nerve damage causes numbness in your foot, which makes normal walking difficult or even impossible.
Sciatica can also potentially cause permanent nerve damage, resulting in a loss of feeling in the affected legs.
Diagnosis and Tests
How is sciatica diagnosed?
A healthcare provider can diagnose sciatica using a combination of methods. They’ll review your medical history and ask about your symptoms. They’ll also do a physical examination. That exam will include:
Walking. Sciatica often causes visible changes in how you walk. Your provider will watch for those changes as part of diagnosing sciatica.
Straight leg raise test. This involves having you lie on an exam table with your legs straight out. They’ll slowly raise your legs one at a time toward the ceiling and ask when you start to feel pain or other symptoms. These can help pinpoint the cause of sciatica and how to manage it.
Other flexibility and strength checks. These can help your provider determine if any other factors are causing or contributing to your sciatica.
What tests will be done to diagnose this condition?
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Sciatica is a very common condition. About 40% of people in the U.S. experience some form of sciatica during their lifetime. It rarely happens before age 20 unless it’s injury-related.
What are the symptoms of sciatica?
Sciatica symptoms can include:
Pain. Sciatica pain happens because of pressure on the affected nerve(s). Most people describe sciatica pain as burning or like an electric shock. This pain also often shoots or radiates down the leg on the affected side. Pain commonly happens with coughing, sneezing, bending or lifting your legs upward when lying on your back.
Tingling or “pins and needles” (paresthesia). This is similar to the feeling you have when a leg falls asleep because you sat cross-legged.
Numbness. This is when you can’t feel sensations on the skin in the affected areas of your back or leg. It happens because signals from your back or leg are having trouble reaching your brain.
Muscle weakness. This is a more severe symptom. It means that muscle command signals are having trouble reaching their destinations in your back or legs.
Urinary incontinence or fecal incontinence. This is a very severe symptom. It means signals that control your bladder and bowels aren’t reaching their destinations.
What causes sciatica?
Sciatica can happen because of any condition that affects the sciatic nerve. It can also happen because of conditions affecting any of the five spinal nerves that bundle to form the sciatic nerve.
Conditions that can cause sciatica include:
Herniated disks.
Degenerative disk disease.
Spinal stenosis.
Foraminal stenosis.
Spondylolisthesis.
Osteoarthritis.
Injuries.
Pregnancy.
Tumors, cysts or other growths.
Conus medullas syndrome.
Cauda equina syndrome.
What are the risk factors for sciatica?
Because sciatica can happen for so many reasons, there are many potential risk factors, which include, but aren’t limited to:
Having a current or previous injury. An injury to your spine or lower back increases your risk of developing sciatica.
Normal wear-and-tear. As you get older, normal wear-and-tear on your spine can lead to pinched nerves, herniated disks and other conditions that can cause sciatica. Age-related conditions like osteoarthritis can also play a role.
Having excess weight or obesity. Your spine is like a construction crane when you stand upright. The weight you carry in the front of your body is what your spine (crane) has to hoist. Muscles in your back are like the winch and cable, pulling to keep you vertical. The more weight you have, the more your back muscles have to work. That can lead to back strains, pain and other issues.
Having insufficient core strength. Your “core” is the term for the muscles of your back and abdomen (stomach area). Like in the crane analogy, having a stronger core is like upgrading the crane’s components to handle a heavier load. The muscles of your abdomen are important because they help anchor your back muscles.
Your job. Jobs that require heavy lifting, a lot of bending, or working in awkward or unusual positions may increase your risk of low back problems. However, jobs with prolonged sitting — especially without proper back support — may also increase your risk of low back problems.
Not using good posture and form when lifting. Even if you’re physically fit and active, you can still be prone to sciatica if you don’t follow proper body form during weight lifting, strength training or similar activities.
Having diabetes. Type 2 diabetes increases your risk of diabetes-related peripheral neuropathy. That damages your nerves, including any of the nerves that can cause or contribute to sciatica.
Physical inactivity. Sitting for long periods and a lack of physical activity can contribute to an increased risk of sciatica.
Using tobacco. Nicotine use can affect circulation and increase your risk of chronic pain. That includes conditions like sciatica.
Unknown causes. Many cases of sciatica don’t have a cause that healthcare providers can find.
What are the complications of sciatica?
Most people recover fully from sciatica. However, a possible complication of sciatica is chronic (long-term) pain.
If there’s serious damage to an affected nerve, chronic muscle weakness, such as a “drop foot,” might happen. That’s when nerve damage causes numbness in your foot, which makes normal walking difficult or even impossible.
Sciatica can also potentially cause permanent nerve damage, resulting in a loss of feeling in the affected legs.
Diagnosis and Tests
How is sciatica diagnosed?
A healthcare provider can diagnose sciatica using a combination of methods. They’ll review your medical history and ask about your symptoms. They’ll also do a physical examination. That exam will include:
Walking. Sciatica often causes visible changes in how you walk. Your provider will watch for those changes as part of diagnosing sciatica.
Straight leg raise test. This involves having you lie on an exam table with your legs straight out. They’ll slowly raise your legs one at a time toward the ceiling and ask when you start to feel pain or other symptoms. These can help pinpoint the cause of sciatica and how to manage it.
Other flexibility and strength checks. These can help your provider determine if any other factors are causing or contributing to your sciatica.
What tests will be done to diagnose this condition?
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
True sciatica. This is any condition or injury that directly affects your sciatic nerve.
Sciatica-like conditions. These are conditions that feel like sciatica, but happen for other reasons related to the sciatic nerve or the nerves that bundle together to form it.
Healthcare providers tend to refer to both types as just “sciatica.” The differences between them usually only matter when your healthcare provider determines how to treat it.
How common is sciatica?
Sciatica is a very common condition. About 40% of people in the U.S. experience some form of sciatica during their lifetime. It rarely happens before age 20 unless it’s injury-related.
What are the symptoms of sciatica?
Sciatica symptoms can include:
Pain. Sciatica pain happens because of pressure on the affected nerve(s). Most people describe sciatica pain as burning or like an electric shock. This pain also often shoots or radiates down the leg on the affected side. Pain commonly happens with coughing, sneezing, bending or lifting your legs upward when lying on your back.
Tingling or “pins and needles” (paresthesia). This is similar to the feeling you have when a leg falls asleep because you sat cross-legged.
Numbness. This is when you can’t feel sensations on the skin in the affected areas of your back or leg. It happens because signals from your back or leg are having trouble reaching your brain.
Muscle weakness. This is a more severe symptom. It means that muscle command signals are having trouble reaching their destinations in your back or legs.
Urinary incontinence or fecal incontinence. This is a very severe symptom. It means signals that control your bladder and bowels aren’t reaching their destinations.
What causes sciatica?
Sciatica can happen because of any condition that affects the sciatic nerve. It can also happen because of conditions affecting any of the five spinal nerves that bundle to form the sciatic nerve.
Conditions that can cause sciatica include:
Herniated disks.
Degenerative disk disease.
Spinal stenosis.
Foraminal stenosis.
Spondylolisthesis.
Osteoarthritis.
Injuries.
Pregnancy.
Tumors, cysts or other growths.
Conus medullas syndrome.
Cauda equina syndrome.
What are the risk factors for sciatica?
Because sciatica can happen for so many reasons, there are many potential risk factors, which include, but aren’t limited to:
Having a current or previous injury. An injury to your spine or lower back increases your risk of developing sciatica.
Normal wear-and-tear. As you get older, normal wear-and-tear on your spine can lead to pinched nerves, herniated disks and other conditions that can cause sciatica. Age-related conditions like osteoarthritis can also play a role.
Having excess weight or obesity. Your spine is like a construction crane when you stand upright. The weight you carry in the front of your body is what your spine (crane) has to hoist. Muscles in your back are like the winch and cable, pulling to keep you vertical. The more weight you have, the more your back muscles have to work. That can lead to back strains, pain and other issues.
Having insufficient core strength. Your “core” is the term for the muscles of your back and abdomen (stomach area). Like in the crane analogy, having a stronger core is like upgrading the crane’s components to handle a heavier load. The muscles of your abdomen are important because they help anchor your back muscles.
Your job. Jobs that require heavy lifting, a lot of bending, or working in awkward or unusual positions may increase your risk of low back problems. However, jobs with prolonged sitting — especially without proper back support — may also increase your risk of low back problems.
Not using good posture and form when lifting. Even if you’re physically fit and active, you can still be prone to sciatica if you don’t follow proper body form during weight lifting, strength training or similar activities.
Having diabetes. Type 2 diabetes increases your risk of diabetes-related peripheral neuropathy. That damages your nerves, including any of the nerves that can cause or contribute to sciatica.
Physical inactivity. Sitting for long periods and a lack of physical activity can contribute to an increased risk of sciatica.
Using tobacco. Nicotine use can affect circulation and increase your risk of chronic pain. That includes conditions like sciatica.
Unknown causes. Many cases of sciatica don’t have a cause that healthcare providers can find.
What are the complications of sciatica?
Most people recover fully from sciatica. However, a possible complication of sciatica is chronic (long-term) pain.
If there’s serious damage to an affected nerve, chronic muscle weakness, such as a “drop foot,” might happen. That’s when nerve damage causes numbness in your foot, which makes normal walking difficult or even impossible.
Sciatica can also potentially cause permanent nerve damage, resulting in a loss of feeling in the affected legs.
Diagnosis and Tests
How is sciatica diagnosed?
A healthcare provider can diagnose sciatica using a combination of methods. They’ll review your medical history and ask about your symptoms. They’ll also do a physical examination. That exam will include:
Walking. Sciatica often causes visible changes in how you walk. Your provider will watch for those changes as part of diagnosing sciatica.
Straight leg raise test. This involves having you lie on an exam table with your legs straight out. They’ll slowly raise your legs one at a time toward the ceiling and ask when you start to feel pain or other symptoms. These can help pinpoint the cause of sciatica and how to manage it.
Other flexibility and strength checks. These can help your provider determine if any other factors are causing or contributing to your sciatica.
What tests will be done to diagnose this condition?
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
There are two types of sciatica. Regardless of what type you have, the effects are the same. The types are:
True sciatica. This is any condition or injury that directly affects your sciatic nerve.
Sciatica-like conditions. These are conditions that feel like sciatica, but happen for other reasons related to the sciatic nerve or the nerves that bundle together to form it.
Healthcare providers tend to refer to both types as just “sciatica.” The differences between them usually only matter when your healthcare provider determines how to treat it.
How common is sciatica?
Sciatica is a very common condition. About 40% of people in the U.S. experience some form of sciatica during their lifetime. It rarely happens before age 20 unless it’s injury-related.
What are the symptoms of sciatica?
Sciatica symptoms can include:
Pain. Sciatica pain happens because of pressure on the affected nerve(s). Most people describe sciatica pain as burning or like an electric shock. This pain also often shoots or radiates down the leg on the affected side. Pain commonly happens with coughing, sneezing, bending or lifting your legs upward when lying on your back.
Tingling or “pins and needles” (paresthesia). This is similar to the feeling you have when a leg falls asleep because you sat cross-legged.
Numbness. This is when you can’t feel sensations on the skin in the affected areas of your back or leg. It happens because signals from your back or leg are having trouble reaching your brain.
Muscle weakness. This is a more severe symptom. It means that muscle command signals are having trouble reaching their destinations in your back or legs.
Urinary incontinence or fecal incontinence. This is a very severe symptom. It means signals that control your bladder and bowels aren’t reaching their destinations.
What causes sciatica?
Sciatica can happen because of any condition that affects the sciatic nerve. It can also happen because of conditions affecting any of the five spinal nerves that bundle to form the sciatic nerve.
Conditions that can cause sciatica include:
Herniated disks.
Degenerative disk disease.
Spinal stenosis.
Foraminal stenosis.
Spondylolisthesis.
Osteoarthritis.
Injuries.
Pregnancy.
Tumors, cysts or other growths.
Conus medullas syndrome.
Cauda equina syndrome.
What are the risk factors for sciatica?
Because sciatica can happen for so many reasons, there are many potential risk factors, which include, but aren’t limited to:
Having a current or previous injury. An injury to your spine or lower back increases your risk of developing sciatica.
Normal wear-and-tear. As you get older, normal wear-and-tear on your spine can lead to pinched nerves, herniated disks and other conditions that can cause sciatica. Age-related conditions like osteoarthritis can also play a role.
Having excess weight or obesity. Your spine is like a construction crane when you stand upright. The weight you carry in the front of your body is what your spine (crane) has to hoist. Muscles in your back are like the winch and cable, pulling to keep you vertical. The more weight you have, the more your back muscles have to work. That can lead to back strains, pain and other issues.
Having insufficient core strength. Your “core” is the term for the muscles of your back and abdomen (stomach area). Like in the crane analogy, having a stronger core is like upgrading the crane’s components to handle a heavier load. The muscles of your abdomen are important because they help anchor your back muscles.
Your job. Jobs that require heavy lifting, a lot of bending, or working in awkward or unusual positions may increase your risk of low back problems. However, jobs with prolonged sitting — especially without proper back support — may also increase your risk of low back problems.
Not using good posture and form when lifting. Even if you’re physically fit and active, you can still be prone to sciatica if you don’t follow proper body form during weight lifting, strength training or similar activities.
Having diabetes. Type 2 diabetes increases your risk of diabetes-related peripheral neuropathy. That damages your nerves, including any of the nerves that can cause or contribute to sciatica.
Physical inactivity. Sitting for long periods and a lack of physical activity can contribute to an increased risk of sciatica.
Using tobacco. Nicotine use can affect circulation and increase your risk of chronic pain. That includes conditions like sciatica.
Unknown causes. Many cases of sciatica don’t have a cause that healthcare providers can find.
What are the complications of sciatica?
Most people recover fully from sciatica. However, a possible complication of sciatica is chronic (long-term) pain.
If there’s serious damage to an affected nerve, chronic muscle weakness, such as a “drop foot,” might happen. That’s when nerve damage causes numbness in your foot, which makes normal walking difficult or even impossible.
Sciatica can also potentially cause permanent nerve damage, resulting in a loss of feeling in the affected legs.
Diagnosis and Tests
How is sciatica diagnosed?
A healthcare provider can diagnose sciatica using a combination of methods. They’ll review your medical history and ask about your symptoms. They’ll also do a physical examination. That exam will include:
Walking. Sciatica often causes visible changes in how you walk. Your provider will watch for those changes as part of diagnosing sciatica.
Straight leg raise test. This involves having you lie on an exam table with your legs straight out. They’ll slowly raise your legs one at a time toward the ceiling and ask when you start to feel pain or other symptoms. These can help pinpoint the cause of sciatica and how to manage it.
Other flexibility and strength checks. These can help your provider determine if any other factors are causing or contributing to your sciatica.
What tests will be done to diagnose this condition?
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Sciatica is nerve pain from an injury or irritation to your sciatic nerve. In addition to pain, it can involve tingling or numbness in your back or butt that may also radiate down your leg. More severe symptoms are also possible.
Your sciatic nerve is the longest and thickest nerve in your body. It’s up to 2 centimeters wide (a U.S. penny or a United Kingdom 1 pence coin are about the same width). Despite its name, it’s not just one nerve. It’s actually a bundle of nerves that come from five nerve roots branching off from your spinal cord.
You have two sciatic nerves, one on each side of your body. Each sciatic nerve runs through your hip and buttock on one side. They each go down the leg on their side of your body until they reach just below your knee. Once there, they split into other nerves that connect to parts farther down, including your lower leg, foot and toes.
Having sciatica means you can experience mild to severe pain anywhere with nerves that connect to the sciatic nerve. The symptoms can affect your lower back, hips, buttocks or legs. Some symptoms may extend as far down as your feet and toes, depending on the specific nerve(s) affected.
Types of sciatica
There are two types of sciatica. Regardless of what type you have, the effects are the same. The types are:
True sciatica. This is any condition or injury that directly affects your sciatic nerve.
Sciatica-like conditions. These are conditions that feel like sciatica, but happen for other reasons related to the sciatic nerve or the nerves that bundle together to form it.
Healthcare providers tend to refer to both types as just “sciatica.” The differences between them usually only matter when your healthcare provider determines how to treat it.
How common is sciatica?
Sciatica is a very common condition. About 40% of people in the U.S. experience some form of sciatica during their lifetime. It rarely happens before age 20 unless it’s injury-related.
What are the symptoms of sciatica?
Sciatica symptoms can include:
Pain. Sciatica pain happens because of pressure on the affected nerve(s). Most people describe sciatica pain as burning or like an electric shock. This pain also often shoots or radiates down the leg on the affected side. Pain commonly happens with coughing, sneezing, bending or lifting your legs upward when lying on your back.
Tingling or “pins and needles” (paresthesia). This is similar to the feeling you have when a leg falls asleep because you sat cross-legged.
Numbness. This is when you can’t feel sensations on the skin in the affected areas of your back or leg. It happens because signals from your back or leg are having trouble reaching your brain.
Muscle weakness. This is a more severe symptom. It means that muscle command signals are having trouble reaching their destinations in your back or legs.
Urinary incontinence or fecal incontinence. This is a very severe symptom. It means signals that control your bladder and bowels aren’t reaching their destinations.
What causes sciatica?
Sciatica can happen because of any condition that affects the sciatic nerve. It can also happen because of conditions affecting any of the five spinal nerves that bundle to form the sciatic nerve.
Conditions that can cause sciatica include:
Herniated disks.
Degenerative disk disease.
Spinal stenosis.
Foraminal stenosis.
Spondylolisthesis.
Osteoarthritis.
Injuries.
Pregnancy.
Tumors, cysts or other growths.
Conus medullas syndrome.
Cauda equina syndrome.
What are the risk factors for sciatica?
Because sciatica can happen for so many reasons, there are many potential risk factors, which include, but aren’t limited to:
Having a current or previous injury. An injury to your spine or lower back increases your risk of developing sciatica.
Normal wear-and-tear. As you get older, normal wear-and-tear on your spine can lead to pinched nerves, herniated disks and other conditions that can cause sciatica. Age-related conditions like osteoarthritis can also play a role.
Having excess weight or obesity. Your spine is like a construction crane when you stand upright. The weight you carry in the front of your body is what your spine (crane) has to hoist. Muscles in your back are like the winch and cable, pulling to keep you vertical. The more weight you have, the more your back muscles have to work. That can lead to back strains, pain and other issues.
Having insufficient core strength. Your “core” is the term for the muscles of your back and abdomen (stomach area). Like in the crane analogy, having a stronger core is like upgrading the crane’s components to handle a heavier load. The muscles of your abdomen are important because they help anchor your back muscles.
Your job. Jobs that require heavy lifting, a lot of bending, or working in awkward or unusual positions may increase your risk of low back problems. However, jobs with prolonged sitting — especially without proper back support — may also increase your risk of low back problems.
Not using good posture and form when lifting. Even if you’re physically fit and active, you can still be prone to sciatica if you don’t follow proper body form during weight lifting, strength training or similar activities.
Having diabetes. Type 2 diabetes increases your risk of diabetes-related peripheral neuropathy. That damages your nerves, including any of the nerves that can cause or contribute to sciatica.
Physical inactivity. Sitting for long periods and a lack of physical activity can contribute to an increased risk of sciatica.
Using tobacco. Nicotine use can affect circulation and increase your risk of chronic pain. That includes conditions like sciatica.
Unknown causes. Many cases of sciatica don’t have a cause that healthcare providers can find.
What are the complications of sciatica?
Most people recover fully from sciatica. However, a possible complication of sciatica is chronic (long-term) pain.
If there’s serious damage to an affected nerve, chronic muscle weakness, such as a “drop foot,” might happen. That’s when nerve damage causes numbness in your foot, which makes normal walking difficult or even impossible.
Sciatica can also potentially cause permanent nerve damage, resulting in a loss of feeling in the affected legs.
Diagnosis and Tests
How is sciatica diagnosed?
A healthcare provider can diagnose sciatica using a combination of methods. They’ll review your medical history and ask about your symptoms. They’ll also do a physical examination. That exam will include:
Walking. Sciatica often causes visible changes in how you walk. Your provider will watch for those changes as part of diagnosing sciatica.
Straight leg raise test. This involves having you lie on an exam table with your legs straight out. They’ll slowly raise your legs one at a time toward the ceiling and ask when you start to feel pain or other symptoms. These can help pinpoint the cause of sciatica and how to manage it.
Other flexibility and strength checks. These can help your provider determine if any other factors are causing or contributing to your sciatica.
What tests will be done to diagnose this condition?
Several tests can help with diagnosing sciatica and ruling out similar conditions. The most common or likely tests include, but aren’t limited to:
Spine X-rays or computed tomography (CT) scans.
Magnetic resonance imaging (MRI) scans.
Nerve conduction velocity studies
Electromyography.
Myelogram.
How is sciatica treated, and is there a cure?
Treating sciatica usually involves trying to decrease pain and increase mobility. Many treatments are things you can do yourself.
There are several treatment options if you have sciatica that won’t go away or is more severe. Surgery might be an option if your case is severe or other treatments don’t help.
Self-treatment
Depending on the cause, milder cases of sciatica usually get better with self-treatment.
NOTE: Pain that’s moderate to severe, with numbness and tingling or muscle weakness are all symptoms that need professional medical care. You shouldn’t try to self-treat them.
Self-treatments can include:
Ice. Cold or ice packs can help reduce pain and swelling during the first few days after sciatica pain starts. You can use an ice pack or a bag of frozen vegetables for this (but always wrap them in a towel to prevent cold-related injuries to your skin). Apply cold for 20 minutes at a time, several times a day.
Heat. After the first several days of using cold or ice, switch to a heating pad or warm compress. Apply heat for 20 minutes at a time. If you’re still in pain, switch between hot and cold packs — whichever best relieves your discomfort.
Over-the-counter medicines. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually the first choice. They reduce pain, swelling and inflammation.
Stretching and activity. Learning how to stretch properly from an instructor with experience with low back pain can be a major help. They may also be able to help you work your way up to other general strengthening, core muscle strengthening and aerobic exercises.
If the self-care treatment approach doesn’t help after a few weeks, you should talk to a healthcare provider.
Conservative treatments
Conservative treatments are a step up from self-treatment. Your healthcare provider can offer these as options if self-care wasn’t helpful or if your symptoms are severe enough to need more involved care.
Conservative treatments can involve similar treatments to self-care, but with your healthcare provider guiding you. They can also involve the following:
Prescription medications. Painkillers, muscle relaxers and other medications may help with sciatica symptoms. Other medications, like tricyclic antidepressants and anti-seizure medications, may also help if you have chronic or nerve-based pain.
Physical therapy. The goal of physical therapy is to find exercise movements that decrease sciatica by reducing pressure on the nerve. Options include stretching exercises or low-impact activities like walking, swimming or water aerobics.
Spinal injections. Injections like corticosteroids may provide short-term relief (typically up to three months). These usually involve local anesthesia, so there’s less discomfort. Your healthcare provider can tell you more about this process.
Alternative therapies. These treatments are increasingly popular and offer options other than standard medical therapies or medications. They include seeing a chiropractor for spine adjustments, yoga, acupuncture and more. Massage therapy might also help muscle spasms that occur with sciatica. Biofeedback can also help you manage pain and relieve stress.
Surgery options for sciatica
Surgery may be the best option when sciatica is more severe. Usually, healthcare providers don’t recommend surgery unless you have symptoms that indicate nerve damage is happening or imminent. They may also recommend surgery if you have severe pain that prevents you from working or going about your usual routine, or if your symptoms don’t improve after six to eight weeks of conservative treatment.
Surgery options to relieve sciatica include:
Diskectomy. This is a surgery that removes fragments or small sections of a herniated disk that are pressing on a nerve.
Laminectomy. Each vertebra has a rear section called the lamina (it’s on the side of the vertebra just underneath the skin of your back). A laminectomy involves removing a section of the lamina that’s pressing on spinal nerves.
What are the possible complications or side effects of treatment?
The possible complications and side effects depend on many factors, especially the specific treatments used, the severity of your symptoms, what caused your sciatica and more. Your healthcare provider is the best person to tell you about the possible side effects and complications that are most likely. They can also advise you on managing, minimizing or avoiding them.
How soon after treatment will I feel better?
Recovery time from sciatica depends on the specific treatment, the severity of your symptoms, their cause and more. Many cases of sciatica go away within four to six weeks without needing professional medical treatment.
More severe cases may also take weeks or months to get better, especially if you have more severe symptoms. Waiting too long to get treatment for sciatica — generally more than six months — also makes a good outcome less likely, so it’s important not to wait too long to talk to a healthcare provider.
Is sciatica preventable?
Some causes of sciatica are preventable, but others happen unpredictably or for unknown reasons. For the causes that aren’t preventable, it may still be possible to reduce your risk of developing them.
The following can help prevent sciatica or reduce the risk of it happening:
Maintain good posture. Follow good posture techniques while you’re sitting, standing, lifting objects and sleeping.
Quit (or don’t start) using tobacco products. Nicotine from any source (including vaping) reduces blood supply to your bones, which can weaken your spine and its various components.
Reach and maintain a weight that’s healthy for you. Your primary care provider can guide you on how to eat and get physical activity. Make sure you get enough calcium and vitamin D for bone health, too.
Stay active. Physical activity can include everything from stretching to strength training. Increasing core strength and flexibility can improve back pain. Other forms of activity, such as aerobic exercise, can also help you reach and maintain a weight that’s healthy for you.
Protect yourself from falls. Wear shoes that fit and keep stairs and walkways free of clutter to reduce your chance of a fall. Make sure rooms are well-lit, and there are grab bars in bathrooms and rails on stairways.
Take time to recover if needed. Don’t try to work through back pain. That can lead to even worse injuries. Back pain doesn’t have to keep you from being active, either. You can still participate in low-impact activities such as swimming, walking, yoga or tai chi.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Grade 0 – No neck pain, stiffness, or any physical signs are noticed.
Grade 1: Neck complaints of pain, stiffness or tenderness only but no physical signs are noted by the examining clinician.
Grade 2: Neck complaints and the examining clinician finds Musculoskeletal signs such as decreased range of movement and point tenderness in the neck.
Grade 3: Neck complaints plus neurological signs such as decreased deep tendon reflexes, weakness and sensory deficits.
Grade 4: Neck complaints and fracture or dislocation, or injury to the spinal cord.
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Whiplash Associated Disorders (WAD) is often graded using the Quebec Task Force classification system which separates them into five different categories:
Grade 0 – No neck pain, stiffness, or any physical signs are noticed.
Grade 1: Neck complaints of pain, stiffness or tenderness only but no physical signs are noted by the examining clinician.
Grade 2: Neck complaints and the examining clinician finds Musculoskeletal signs such as decreased range of movement and point tenderness in the neck.
Grade 3: Neck complaints plus neurological signs such as decreased deep tendon reflexes, weakness and sensory deficits.
Grade 4: Neck complaints and fracture or dislocation, or injury to the spinal cord.
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Whiplash Associated Disorders (WAD) is often graded using the Quebec Task Force classification system which separates them into five different categories:
Grade 0 – No neck pain, stiffness, or any physical signs are noticed.
Grade 1: Neck complaints of pain, stiffness or tenderness only but no physical signs are noted by the examining clinician.
Grade 2: Neck complaints and the examining clinician finds Musculoskeletal signs such as decreased range of movement and point tenderness in the neck.
Grade 3: Neck complaints plus neurological signs such as decreased deep tendon reflexes, weakness and sensory deficits.
Grade 4: Neck complaints and fracture or dislocation, or injury to the spinal cord.
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Checking range of motion in your neck, upper back and shoulders.
Gently palpating the areas affected in your neck, shoulders or back, to feel for pain and tenderness.
Assessing your reflexes, strength and sensation in your limbs – this will assess your nerves.
Looking at other areas of your spine and peripheral joints that might also be contributing or causing your symptoms.
Observe specific movements and actions to assess any movement impairments or functional limitations
Whiplash Associated Disorders (WAD) is often graded using the Quebec Task Force classification system which separates them into five different categories:
Grade 0 – No neck pain, stiffness, or any physical signs are noticed.
Grade 1: Neck complaints of pain, stiffness or tenderness only but no physical signs are noted by the examining clinician.
Grade 2: Neck complaints and the examining clinician finds Musculoskeletal signs such as decreased range of movement and point tenderness in the neck.
Grade 3: Neck complaints plus neurological signs such as decreased deep tendon reflexes, weakness and sensory deficits.
Grade 4: Neck complaints and fracture or dislocation, or injury to the spinal cord.
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Because your neck is a complex structure with lots of moving parts, your Physio will need to spend time doing a thorough physical examination, in order to figure out exactly which areas have been affected.
Your physical assessment will likely include:
Checking range of motion in your neck, upper back and shoulders.
Gently palpating the areas affected in your neck, shoulders or back, to feel for pain and tenderness.
Assessing your reflexes, strength and sensation in your limbs – this will assess your nerves.
Looking at other areas of your spine and peripheral joints that might also be contributing or causing your symptoms.
Observe specific movements and actions to assess any movement impairments or functional limitations
Whiplash Associated Disorders (WAD) is often graded using the Quebec Task Force classification system which separates them into five different categories:
Grade 0 – No neck pain, stiffness, or any physical signs are noticed.
Grade 1: Neck complaints of pain, stiffness or tenderness only but no physical signs are noted by the examining clinician.
Grade 2: Neck complaints and the examining clinician finds Musculoskeletal signs such as decreased range of movement and point tenderness in the neck.
Grade 3: Neck complaints plus neurological signs such as decreased deep tendon reflexes, weakness and sensory deficits.
Grade 4: Neck complaints and fracture or dislocation, or injury to the spinal cord.
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
At Complete all of our Physiotherapists are highly skilled diagnosticians, and will be able to give you a clear diagnosis and explanation of your condition following your initial assessment. They will take you through a full subjective interview followed by a comprehensive physical and neurological examination, to evaluate the cause and extent of your symptoms.
Because your neck is a complex structure with lots of moving parts, your Physio will need to spend time doing a thorough physical examination, in order to figure out exactly which areas have been affected.
Your physical assessment will likely include:
Checking range of motion in your neck, upper back and shoulders.
Gently palpating the areas affected in your neck, shoulders or back, to feel for pain and tenderness.
Assessing your reflexes, strength and sensation in your limbs – this will assess your nerves.
Looking at other areas of your spine and peripheral joints that might also be contributing or causing your symptoms.
Observe specific movements and actions to assess any movement impairments or functional limitations
Whiplash Associated Disorders (WAD) is often graded using the Quebec Task Force classification system which separates them into five different categories:
Grade 0 – No neck pain, stiffness, or any physical signs are noticed.
Grade 1: Neck complaints of pain, stiffness or tenderness only but no physical signs are noted by the examining clinician.
Grade 2: Neck complaints and the examining clinician finds Musculoskeletal signs such as decreased range of movement and point tenderness in the neck.
Grade 3: Neck complaints plus neurological signs such as decreased deep tendon reflexes, weakness and sensory deficits.
Grade 4: Neck complaints and fracture or dislocation, or injury to the spinal cord.
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
The symptoms of whiplash may look like other neck conditions and medical problems; therefore it is very important to see an experienced healthcare professional to get an accurate diagnosis. If you have any of the above symptoms or are concerned that you have a whiplash injury then please get in touch with us at Complete, to book an appointment.
Please note that injuries or accidents that cause whiplash can also result in concussion. Since concussions can be serious, you need to seek urgent medical care if you have a severe headache that worsens or persists, you have trouble talking, problems with balance or coordination, or are confused, dizzy, nauseous, excessively sleepy, or have been unconscious.
How do we Diagnose Whiplash?
At Complete all of our Physiotherapists are highly skilled diagnosticians, and will be able to give you a clear diagnosis and explanation of your condition following your initial assessment. They will take you through a full subjective interview followed by a comprehensive physical and neurological examination, to evaluate the cause and extent of your symptoms.
Because your neck is a complex structure with lots of moving parts, your Physio will need to spend time doing a thorough physical examination, in order to figure out exactly which areas have been affected.
Your physical assessment will likely include:
Checking range of motion in your neck, upper back and shoulders.
Gently palpating the areas affected in your neck, shoulders or back, to feel for pain and tenderness.
Assessing your reflexes, strength and sensation in your limbs – this will assess your nerves.
Looking at other areas of your spine and peripheral joints that might also be contributing or causing your symptoms.
Observe specific movements and actions to assess any movement impairments or functional limitations
Whiplash Associated Disorders (WAD) is often graded using the Quebec Task Force classification system which separates them into five different categories:
Grade 0 – No neck pain, stiffness, or any physical signs are noticed.
Grade 1: Neck complaints of pain, stiffness or tenderness only but no physical signs are noted by the examining clinician.
Grade 2: Neck complaints and the examining clinician finds Musculoskeletal signs such as decreased range of movement and point tenderness in the neck.
Grade 3: Neck complaints plus neurological signs such as decreased deep tendon reflexes, weakness and sensory deficits.
Grade 4: Neck complaints and fracture or dislocation, or injury to the spinal cord.
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Headaches – often starting at the base of the skull
Tenderness or pain in the muscles around the neck, shoulders, upper back or arms
Tingling or numbness in the arms or hands
Fatigue
Dizziness
Some people also experience:
Problems with vision – blurred or double vision
Tinnitus – ringing in the ears
Pain in the jaw
Pain when swallowing
Difficulty Sleeping
Irritability, Anxiety or Depression
Difficulty concentrating or problems with memory
The symptoms of whiplash may look like other neck conditions and medical problems; therefore it is very important to see an experienced healthcare professional to get an accurate diagnosis. If you have any of the above symptoms or are concerned that you have a whiplash injury then please get in touch with us at Complete, to book an appointment.
Please note that injuries or accidents that cause whiplash can also result in concussion. Since concussions can be serious, you need to seek urgent medical care if you have a severe headache that worsens or persists, you have trouble talking, problems with balance or coordination, or are confused, dizzy, nauseous, excessively sleepy, or have been unconscious.
How do we Diagnose Whiplash?
At Complete all of our Physiotherapists are highly skilled diagnosticians, and will be able to give you a clear diagnosis and explanation of your condition following your initial assessment. They will take you through a full subjective interview followed by a comprehensive physical and neurological examination, to evaluate the cause and extent of your symptoms.
Because your neck is a complex structure with lots of moving parts, your Physio will need to spend time doing a thorough physical examination, in order to figure out exactly which areas have been affected.
Your physical assessment will likely include:
Checking range of motion in your neck, upper back and shoulders.
Gently palpating the areas affected in your neck, shoulders or back, to feel for pain and tenderness.
Assessing your reflexes, strength and sensation in your limbs – this will assess your nerves.
Looking at other areas of your spine and peripheral joints that might also be contributing or causing your symptoms.
Observe specific movements and actions to assess any movement impairments or functional limitations
Whiplash Associated Disorders (WAD) is often graded using the Quebec Task Force classification system which separates them into five different categories:
Grade 0 – No neck pain, stiffness, or any physical signs are noticed.
Grade 1: Neck complaints of pain, stiffness or tenderness only but no physical signs are noted by the examining clinician.
Grade 2: Neck complaints and the examining clinician finds Musculoskeletal signs such as decreased range of movement and point tenderness in the neck.
Grade 3: Neck complaints plus neurological signs such as decreased deep tendon reflexes, weakness and sensory deficits.
Grade 4: Neck complaints and fracture or dislocation, or injury to the spinal cord.
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Sometimes the pain from whiplash/neck strain is felt immediately. In other cases, symptoms can take several hours or days to appear, so it’s important to pay attention to any physical changes for a few days after any crash, fall or traumatic event.
Signs and symptoms of whiplash may include some or all of the below:
Neck pain and stiffness
Increased pain with neck movement
Loss of movement in the neck
Headaches – often starting at the base of the skull
Tenderness or pain in the muscles around the neck, shoulders, upper back or arms
Tingling or numbness in the arms or hands
Fatigue
Dizziness
Some people also experience:
Problems with vision – blurred or double vision
Tinnitus – ringing in the ears
Pain in the jaw
Pain when swallowing
Difficulty Sleeping
Irritability, Anxiety or Depression
Difficulty concentrating or problems with memory
The symptoms of whiplash may look like other neck conditions and medical problems; therefore it is very important to see an experienced healthcare professional to get an accurate diagnosis. If you have any of the above symptoms or are concerned that you have a whiplash injury then please get in touch with us at Complete, to book an appointment.
Please note that injuries or accidents that cause whiplash can also result in concussion. Since concussions can be serious, you need to seek urgent medical care if you have a severe headache that worsens or persists, you have trouble talking, problems with balance or coordination, or are confused, dizzy, nauseous, excessively sleepy, or have been unconscious.
How do we Diagnose Whiplash?
At Complete all of our Physiotherapists are highly skilled diagnosticians, and will be able to give you a clear diagnosis and explanation of your condition following your initial assessment. They will take you through a full subjective interview followed by a comprehensive physical and neurological examination, to evaluate the cause and extent of your symptoms.
Because your neck is a complex structure with lots of moving parts, your Physio will need to spend time doing a thorough physical examination, in order to figure out exactly which areas have been affected.
Your physical assessment will likely include:
Checking range of motion in your neck, upper back and shoulders.
Gently palpating the areas affected in your neck, shoulders or back, to feel for pain and tenderness.
Assessing your reflexes, strength and sensation in your limbs – this will assess your nerves.
Looking at other areas of your spine and peripheral joints that might also be contributing or causing your symptoms.
Observe specific movements and actions to assess any movement impairments or functional limitations
Whiplash Associated Disorders (WAD) is often graded using the Quebec Task Force classification system which separates them into five different categories:
Grade 0 – No neck pain, stiffness, or any physical signs are noticed.
Grade 1: Neck complaints of pain, stiffness or tenderness only but no physical signs are noted by the examining clinician.
Grade 2: Neck complaints and the examining clinician finds Musculoskeletal signs such as decreased range of movement and point tenderness in the neck.
Grade 3: Neck complaints plus neurological signs such as decreased deep tendon reflexes, weakness and sensory deficits.
Grade 4: Neck complaints and fracture or dislocation, or injury to the spinal cord.
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Physical abuse, such as being struck on the head or shaken
Contact sports, such as rugby, boxing, and some martial arts
Horseback riding – falling from a horse
Cycling collisions or falls
Roller Coasters
It can be more serious in older adults (over age 65) due to age-related muscle and bone deterioration and weakening, making them more susceptible to significant muscle and bone injuries of any kind.
What are the Symptoms of Whiplash/ Neck Sprain?
Sometimes the pain from whiplash/neck strain is felt immediately. In other cases, symptoms can take several hours or days to appear, so it’s important to pay attention to any physical changes for a few days after any crash, fall or traumatic event.
Signs and symptoms of whiplash may include some or all of the below:
Neck pain and stiffness
Increased pain with neck movement
Loss of movement in the neck
Headaches – often starting at the base of the skull
Tenderness or pain in the muscles around the neck, shoulders, upper back or arms
Tingling or numbness in the arms or hands
Fatigue
Dizziness
Some people also experience:
Problems with vision – blurred or double vision
Tinnitus – ringing in the ears
Pain in the jaw
Pain when swallowing
Difficulty Sleeping
Irritability, Anxiety or Depression
Difficulty concentrating or problems with memory
The symptoms of whiplash may look like other neck conditions and medical problems; therefore it is very important to see an experienced healthcare professional to get an accurate diagnosis. If you have any of the above symptoms or are concerned that you have a whiplash injury then please get in touch with us at Complete, to book an appointment.
Please note that injuries or accidents that cause whiplash can also result in concussion. Since concussions can be serious, you need to seek urgent medical care if you have a severe headache that worsens or persists, you have trouble talking, problems with balance or coordination, or are confused, dizzy, nauseous, excessively sleepy, or have been unconscious.
How do we Diagnose Whiplash?
At Complete all of our Physiotherapists are highly skilled diagnosticians, and will be able to give you a clear diagnosis and explanation of your condition following your initial assessment. They will take you through a full subjective interview followed by a comprehensive physical and neurological examination, to evaluate the cause and extent of your symptoms.
Because your neck is a complex structure with lots of moving parts, your Physio will need to spend time doing a thorough physical examination, in order to figure out exactly which areas have been affected.
Your physical assessment will likely include:
Checking range of motion in your neck, upper back and shoulders.
Gently palpating the areas affected in your neck, shoulders or back, to feel for pain and tenderness.
Assessing your reflexes, strength and sensation in your limbs – this will assess your nerves.
Looking at other areas of your spine and peripheral joints that might also be contributing or causing your symptoms.
Observe specific movements and actions to assess any movement impairments or functional limitations
Whiplash Associated Disorders (WAD) is often graded using the Quebec Task Force classification system which separates them into five different categories:
Grade 0 – No neck pain, stiffness, or any physical signs are noticed.
Grade 1: Neck complaints of pain, stiffness or tenderness only but no physical signs are noted by the examining clinician.
Grade 2: Neck complaints and the examining clinician finds Musculoskeletal signs such as decreased range of movement and point tenderness in the neck.
Grade 3: Neck complaints plus neurological signs such as decreased deep tendon reflexes, weakness and sensory deficits.
Grade 4: Neck complaints and fracture or dislocation, or injury to the spinal cord.
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Most whiplash injuries result from a collision that produces sudden, acceleration or deceleration forces. Commonly it is an injury often sustained from car accidents, but they also occur frequently in sports, particularly contact sports, and from trips and falls.
The sudden, excessive, forwards and backwards motion during a whiplash injury, causes the soft tissues (muscles, ligaments, and tendons) in the front and back of your neck to be overstretched, and can sometimes cause small tears. Plus, the abnormal compression and shearing forces put on your cervical spine can potentially damage intervertebral discs, facet joints, and even cause fractures to the vertebral bones. This trauma results in significant pain, stiffness and inflammation.
The sharper and stronger the movement, the greater the force on your neck. That’s why whiplash injuries can range from minor to severe. However, even weak levels of force can still cause moderate or severe whiplash.
At its worst, whiplash can cause a break (known as a fracture) in the vertebrae in your neck, creating a risk of damage to your spinal cord and its network of peripheral nerves.
Some events that can cause whiplash include:
Car accidents/collisions
Physical abuse, such as being struck on the head or shaken
Contact sports, such as rugby, boxing, and some martial arts
Horseback riding – falling from a horse
Cycling collisions or falls
Roller Coasters
It can be more serious in older adults (over age 65) due to age-related muscle and bone deterioration and weakening, making them more susceptible to significant muscle and bone injuries of any kind.
What are the Symptoms of Whiplash/ Neck Sprain?
Sometimes the pain from whiplash/neck strain is felt immediately. In other cases, symptoms can take several hours or days to appear, so it’s important to pay attention to any physical changes for a few days after any crash, fall or traumatic event.
Signs and symptoms of whiplash may include some or all of the below:
Neck pain and stiffness
Increased pain with neck movement
Loss of movement in the neck
Headaches – often starting at the base of the skull
Tenderness or pain in the muscles around the neck, shoulders, upper back or arms
Tingling or numbness in the arms or hands
Fatigue
Dizziness
Some people also experience:
Problems with vision – blurred or double vision
Tinnitus – ringing in the ears
Pain in the jaw
Pain when swallowing
Difficulty Sleeping
Irritability, Anxiety or Depression
Difficulty concentrating or problems with memory
The symptoms of whiplash may look like other neck conditions and medical problems; therefore it is very important to see an experienced healthcare professional to get an accurate diagnosis. If you have any of the above symptoms or are concerned that you have a whiplash injury then please get in touch with us at Complete, to book an appointment.
Please note that injuries or accidents that cause whiplash can also result in concussion. Since concussions can be serious, you need to seek urgent medical care if you have a severe headache that worsens or persists, you have trouble talking, problems with balance or coordination, or are confused, dizzy, nauseous, excessively sleepy, or have been unconscious.
How do we Diagnose Whiplash?
At Complete all of our Physiotherapists are highly skilled diagnosticians, and will be able to give you a clear diagnosis and explanation of your condition following your initial assessment. They will take you through a full subjective interview followed by a comprehensive physical and neurological examination, to evaluate the cause and extent of your symptoms.
Because your neck is a complex structure with lots of moving parts, your Physio will need to spend time doing a thorough physical examination, in order to figure out exactly which areas have been affected.
Your physical assessment will likely include:
Checking range of motion in your neck, upper back and shoulders.
Gently palpating the areas affected in your neck, shoulders or back, to feel for pain and tenderness.
Assessing your reflexes, strength and sensation in your limbs – this will assess your nerves.
Looking at other areas of your spine and peripheral joints that might also be contributing or causing your symptoms.
Observe specific movements and actions to assess any movement impairments or functional limitations
Whiplash Associated Disorders (WAD) is often graded using the Quebec Task Force classification system which separates them into five different categories:
Grade 0 – No neck pain, stiffness, or any physical signs are noticed.
Grade 1: Neck complaints of pain, stiffness or tenderness only but no physical signs are noted by the examining clinician.
Grade 2: Neck complaints and the examining clinician finds Musculoskeletal signs such as decreased range of movement and point tenderness in the neck.
Grade 3: Neck complaints plus neurological signs such as decreased deep tendon reflexes, weakness and sensory deficits.
Grade 4: Neck complaints and fracture or dislocation, or injury to the spinal cord.
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
The neck is incredibly complex; it consists of 7 cervical vertebrae (C1-C7), C1 is closest to the skull, while C7 is at the base of the neck. In between each vertebrae are tough, fibrous, shock-absorbing pads called the intervertebral discs. Your cervical spine (neck) also houses the upper portion of the spinal cord through the spinal canal, as well as having an elaborate system of nerves, over 30 muscles, and numerous ligaments and tendons. This means that there are a lot of parts that can be damaged from a whiplash injury.
Your neck naturally compresses, extends, and twists, and acts as a shock absorber for the brain, to ensure minimal damage to the brain from any sudden movement. The cervical spine allows your head to move in nearly every direction; 90° of forward flexion, 90° of backward extension, approx. 180° of rotation side to side, and almost 120° of tilt to either shoulder. Unfortunately, this flexibility makes the neck very susceptible to injury.
The neck also has to support the weight of your head (approx. 5kg); when this weight whips forwards and back at speed, the force that goes through the cervical spine is considerable.
What Causes Whiplash Injury?
Most whiplash injuries result from a collision that produces sudden, acceleration or deceleration forces. Commonly it is an injury often sustained from car accidents, but they also occur frequently in sports, particularly contact sports, and from trips and falls.
The sudden, excessive, forwards and backwards motion during a whiplash injury, causes the soft tissues (muscles, ligaments, and tendons) in the front and back of your neck to be overstretched, and can sometimes cause small tears. Plus, the abnormal compression and shearing forces put on your cervical spine can potentially damage intervertebral discs, facet joints, and even cause fractures to the vertebral bones. This trauma results in significant pain, stiffness and inflammation.
The sharper and stronger the movement, the greater the force on your neck. That’s why whiplash injuries can range from minor to severe. However, even weak levels of force can still cause moderate or severe whiplash.
At its worst, whiplash can cause a break (known as a fracture) in the vertebrae in your neck, creating a risk of damage to your spinal cord and its network of peripheral nerves.
Some events that can cause whiplash include:
Car accidents/collisions
Physical abuse, such as being struck on the head or shaken
Contact sports, such as rugby, boxing, and some martial arts
Horseback riding – falling from a horse
Cycling collisions or falls
Roller Coasters
It can be more serious in older adults (over age 65) due to age-related muscle and bone deterioration and weakening, making them more susceptible to significant muscle and bone injuries of any kind.
What are the Symptoms of Whiplash/ Neck Sprain?
Sometimes the pain from whiplash/neck strain is felt immediately. In other cases, symptoms can take several hours or days to appear, so it’s important to pay attention to any physical changes for a few days after any crash, fall or traumatic event.
Signs and symptoms of whiplash may include some or all of the below:
Neck pain and stiffness
Increased pain with neck movement
Loss of movement in the neck
Headaches – often starting at the base of the skull
Tenderness or pain in the muscles around the neck, shoulders, upper back or arms
Tingling or numbness in the arms or hands
Fatigue
Dizziness
Some people also experience:
Problems with vision – blurred or double vision
Tinnitus – ringing in the ears
Pain in the jaw
Pain when swallowing
Difficulty Sleeping
Irritability, Anxiety or Depression
Difficulty concentrating or problems with memory
The symptoms of whiplash may look like other neck conditions and medical problems; therefore it is very important to see an experienced healthcare professional to get an accurate diagnosis. If you have any of the above symptoms or are concerned that you have a whiplash injury then please get in touch with us at Complete, to book an appointment.
Please note that injuries or accidents that cause whiplash can also result in concussion. Since concussions can be serious, you need to seek urgent medical care if you have a severe headache that worsens or persists, you have trouble talking, problems with balance or coordination, or are confused, dizzy, nauseous, excessively sleepy, or have been unconscious.
How do we Diagnose Whiplash?
At Complete all of our Physiotherapists are highly skilled diagnosticians, and will be able to give you a clear diagnosis and explanation of your condition following your initial assessment. They will take you through a full subjective interview followed by a comprehensive physical and neurological examination, to evaluate the cause and extent of your symptoms.
Because your neck is a complex structure with lots of moving parts, your Physio will need to spend time doing a thorough physical examination, in order to figure out exactly which areas have been affected.
Your physical assessment will likely include:
Checking range of motion in your neck, upper back and shoulders.
Gently palpating the areas affected in your neck, shoulders or back, to feel for pain and tenderness.
Assessing your reflexes, strength and sensation in your limbs – this will assess your nerves.
Looking at other areas of your spine and peripheral joints that might also be contributing or causing your symptoms.
Observe specific movements and actions to assess any movement impairments or functional limitations
Whiplash Associated Disorders (WAD) is often graded using the Quebec Task Force classification system which separates them into five different categories:
Grade 0 – No neck pain, stiffness, or any physical signs are noticed.
Grade 1: Neck complaints of pain, stiffness or tenderness only but no physical signs are noted by the examining clinician.
Grade 2: Neck complaints and the examining clinician finds Musculoskeletal signs such as decreased range of movement and point tenderness in the neck.
Grade 3: Neck complaints plus neurological signs such as decreased deep tendon reflexes, weakness and sensory deficits.
Grade 4: Neck complaints and fracture or dislocation, or injury to the spinal cord.
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Whiplash is a neck injury caused by a sudden, forceful, back-and-forth movement of the neck at speed, resulting in the neck bending beyond its normal range of movement. The injury usually involves the bones and soft tissues in your neck. The whiplash may occur due to a road traffic incident, falling off your bike or off a step or a sporting injury e.g. a rugby tackle.
The majority of whiplash injuries are not thought to be serious, and usually recover well with Physiotherapy, however if left untreated it can lead to long-term pain, discomfort and reduced function.
Anatomy of the Neck
The neck is incredibly complex; it consists of 7 cervical vertebrae (C1-C7), C1 is closest to the skull, while C7 is at the base of the neck. In between each vertebrae are tough, fibrous, shock-absorbing pads called the intervertebral discs. Your cervical spine (neck) also houses the upper portion of the spinal cord through the spinal canal, as well as having an elaborate system of nerves, over 30 muscles, and numerous ligaments and tendons. This means that there are a lot of parts that can be damaged from a whiplash injury.
Your neck naturally compresses, extends, and twists, and acts as a shock absorber for the brain, to ensure minimal damage to the brain from any sudden movement. The cervical spine allows your head to move in nearly every direction; 90° of forward flexion, 90° of backward extension, approx. 180° of rotation side to side, and almost 120° of tilt to either shoulder. Unfortunately, this flexibility makes the neck very susceptible to injury.
The neck also has to support the weight of your head (approx. 5kg); when this weight whips forwards and back at speed, the force that goes through the cervical spine is considerable.
What Causes Whiplash Injury?
Most whiplash injuries result from a collision that produces sudden, acceleration or deceleration forces. Commonly it is an injury often sustained from car accidents, but they also occur frequently in sports, particularly contact sports, and from trips and falls.
The sudden, excessive, forwards and backwards motion during a whiplash injury, causes the soft tissues (muscles, ligaments, and tendons) in the front and back of your neck to be overstretched, and can sometimes cause small tears. Plus, the abnormal compression and shearing forces put on your cervical spine can potentially damage intervertebral discs, facet joints, and even cause fractures to the vertebral bones. This trauma results in significant pain, stiffness and inflammation.
The sharper and stronger the movement, the greater the force on your neck. That’s why whiplash injuries can range from minor to severe. However, even weak levels of force can still cause moderate or severe whiplash.
At its worst, whiplash can cause a break (known as a fracture) in the vertebrae in your neck, creating a risk of damage to your spinal cord and its network of peripheral nerves.
Some events that can cause whiplash include:
Car accidents/collisions
Physical abuse, such as being struck on the head or shaken
Contact sports, such as rugby, boxing, and some martial arts
Horseback riding – falling from a horse
Cycling collisions or falls
Roller Coasters
It can be more serious in older adults (over age 65) due to age-related muscle and bone deterioration and weakening, making them more susceptible to significant muscle and bone injuries of any kind.
What are the Symptoms of Whiplash/ Neck Sprain?
Sometimes the pain from whiplash/neck strain is felt immediately. In other cases, symptoms can take several hours or days to appear, so it’s important to pay attention to any physical changes for a few days after any crash, fall or traumatic event.
Signs and symptoms of whiplash may include some or all of the below:
Neck pain and stiffness
Increased pain with neck movement
Loss of movement in the neck
Headaches – often starting at the base of the skull
Tenderness or pain in the muscles around the neck, shoulders, upper back or arms
Tingling or numbness in the arms or hands
Fatigue
Dizziness
Some people also experience:
Problems with vision – blurred or double vision
Tinnitus – ringing in the ears
Pain in the jaw
Pain when swallowing
Difficulty Sleeping
Irritability, Anxiety or Depression
Difficulty concentrating or problems with memory
The symptoms of whiplash may look like other neck conditions and medical problems; therefore it is very important to see an experienced healthcare professional to get an accurate diagnosis. If you have any of the above symptoms or are concerned that you have a whiplash injury then please get in touch with us at Complete, to book an appointment.
Please note that injuries or accidents that cause whiplash can also result in concussion. Since concussions can be serious, you need to seek urgent medical care if you have a severe headache that worsens or persists, you have trouble talking, problems with balance or coordination, or are confused, dizzy, nauseous, excessively sleepy, or have been unconscious.
How do we Diagnose Whiplash?
At Complete all of our Physiotherapists are highly skilled diagnosticians, and will be able to give you a clear diagnosis and explanation of your condition following your initial assessment. They will take you through a full subjective interview followed by a comprehensive physical and neurological examination, to evaluate the cause and extent of your symptoms.
Because your neck is a complex structure with lots of moving parts, your Physio will need to spend time doing a thorough physical examination, in order to figure out exactly which areas have been affected.
Your physical assessment will likely include:
Checking range of motion in your neck, upper back and shoulders.
Gently palpating the areas affected in your neck, shoulders or back, to feel for pain and tenderness.
Assessing your reflexes, strength and sensation in your limbs – this will assess your nerves.
Looking at other areas of your spine and peripheral joints that might also be contributing or causing your symptoms.
Observe specific movements and actions to assess any movement impairments or functional limitations
Whiplash Associated Disorders (WAD) is often graded using the Quebec Task Force classification system which separates them into five different categories:
Grade 0 – No neck pain, stiffness, or any physical signs are noticed.
Grade 1: Neck complaints of pain, stiffness or tenderness only but no physical signs are noted by the examining clinician.
Grade 2: Neck complaints and the examining clinician finds Musculoskeletal signs such as decreased range of movement and point tenderness in the neck.
Grade 3: Neck complaints plus neurological signs such as decreased deep tendon reflexes, weakness and sensory deficits.
Grade 4: Neck complaints and fracture or dislocation, or injury to the spinal cord.
Depending on your symptoms and what your physiotherapist finds during the physical exam, they may also suggest diagnostic imaging/scans.
X-ray. – This will look at your bones to determine whether there are any vertebral fractures.
MRI or CT scan – Can assess the condition of the cervical spine’s soft tissues (intervertebral discs, muscles, ligaments).
At Complete Physio we have a unique team of physiotherapists who are experts in the treatment and management of whiplash. You are not required to have a GP referral.
How do we treat Whiplash?
There are a number of treatment options that your physiotherapist will discuss with you, and together you will work out a treatment plan based on the source of your symptoms, and your own, personal goals.
Your treatment will likely include some or all of the following:
1. Pain Relief & Protection
Managing your neck pain will likely be the first step in your treatment. Various tools can be used such as medications, ice or heat packs, neck taping techniques, soft tissue massage and acupuncture.
Neck Brace and Taping
A neck brace or a soft collar are rarely advised these days if you are suffering with neck pain, unless you have broken your neck. We often encourage an early range of movement exercises.
Sports taping can be applied to offload muscles and nerves, and help reduce pain.
Soft Tissue Massage
Massage is incredibly useful to help reduce muscle spasms, tension and improve the range of movement of your neck. It also has relaxation benefits.
Acupuncture or Dry Needling
Acupuncture has been used for thousands of years to help with pain and muscle spasm Acupunture is supported by scientific evidence for the treatment of whiplash and neck pain and can be a very effective treatment option.
Medication
Medications are often prescribed to help with the treatment of whiplash. The most common kinds of medications providers prescribe include painkillers, nonsteroidal anti-inflammatory drugs, muscle relaxers and nerve blocks. You should always seek professional medical advice before taking any medication.
2. Regaining Normal Range of Movement and Strength
As your neck pain settles, your physiotherapist will focus on treatments and exercises to ensure you regain your normal neck movement, muscle length, strength, and endurance.
What are the symptoms of neck muscle injuries?
Neck Stretches
You will be given stretching exercises to improve joint range and muscle length. Your physio will also likely do some gentle ‘hands on’ joint mobilisations to work on any localised joint stiffness in the spine.
Your physiotherapist will also assess your movement pattern and posture, and correct any abnormalities.
Strength and Endurance
You will commence a strengthening programme that specifically focuses on neck stability, and targets the deep neck muscles that dynamically control and stabilise your neck. You will also work on global muscle strength, around your upper back, shoulders and arms.
Restoring Full Function
Depending on your occupation, or chosen sport or activities, your physiotherapist will tailor your rehabilitation to work on specific tasks or functional movements, to allow you to return to your desired activities safely.
Spinal injections and Surgery For Whiplash
In very rare cases, an injury from whiplash requires injection therapy or surgery. Spinal injections involve injecting a small amount of steroid (also known as cortisone or corticosteroid) using X-ray guidance (known as fluoroscopy guidance) into the joints and/or soft tissues. Injections are reserved for those cases where the pain is not improving. Surgery is usually only required if there are torn ligaments or fractured vertebrae. Spine surgery will stabilise the affected areas of your spine, preventing nerve damage and further pain.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you would like to speak to Physiotherapists or to book an appointment please call 786-475-3094 or email: info@drabbate.com
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Over-the-counter (OTC) medication may help treat the pain associated with intercostal neuralgia. Some of these medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Treatment for intercostal neuralgia depends on the underlying cause and may include over-the-counter (OTC) and prescription medications and medical procedures.
OTC Medication
Over-the-counter (OTC) medication may help treat the pain associated with intercostal neuralgia. Some of these medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Exercise stress testing: Sometimes called a treadmill test, this test helps your healthcare provider figure out how much the heart can handle with exertion. As the body works harder, it needs more oxygen so it must pump more blood. The stress test can show if the blood supply to the arteries supporting the heart is reduced.
Electrocardiogram: An electrocardiogram is a simple, painless test that measures the electrical activity of the heart.
Echocardiography: This test uses sound waves to produce live images of the heart to help your healthcare provider understand how your heart and its valves are functioning.
Bloodwork: Measures levels of certain cardiac enzymes. If cardiac enzymes are increased, this may indicate a problem with the heart.
Treatment
Treatment for intercostal neuralgia depends on the underlying cause and may include over-the-counter (OTC) and prescription medications and medical procedures.
OTC Medication
Over-the-counter (OTC) medication may help treat the pain associated with intercostal neuralgia. Some of these medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
If you have risk factors for heart disease, such as diabetes, high blood pressure, a history of smoking, or a family history of heart disease, your healthcare provider will want to test your heart function.
Testing may include:
Exercise stress testing: Sometimes called a treadmill test, this test helps your healthcare provider figure out how much the heart can handle with exertion. As the body works harder, it needs more oxygen so it must pump more blood. The stress test can show if the blood supply to the arteries supporting the heart is reduced.
Electrocardiogram: An electrocardiogram is a simple, painless test that measures the electrical activity of the heart.
Echocardiography: This test uses sound waves to produce live images of the heart to help your healthcare provider understand how your heart and its valves are functioning.
Bloodwork: Measures levels of certain cardiac enzymes. If cardiac enzymes are increased, this may indicate a problem with the heart.
Treatment
Treatment for intercostal neuralgia depends on the underlying cause and may include over-the-counter (OTC) and prescription medications and medical procedures.
OTC Medication
Over-the-counter (OTC) medication may help treat the pain associated with intercostal neuralgia. Some of these medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Chest X-ray: Can look for sources of chest, rib, and back pain and find problems in the airways, bones, heart, or lungs.
Nerve conduction velocity testing: Assesses nerve damage and dysfunction.
Electromyography: Evaluates the muscles and nerve cells that control them.
Musculoskeletal ultrasound: Involves more in-depth imaging than traditional X-rays or other imaging studies.
If you have risk factors for heart disease, such as diabetes, high blood pressure, a history of smoking, or a family history of heart disease, your healthcare provider will want to test your heart function.
Testing may include:
Exercise stress testing: Sometimes called a treadmill test, this test helps your healthcare provider figure out how much the heart can handle with exertion. As the body works harder, it needs more oxygen so it must pump more blood. The stress test can show if the blood supply to the arteries supporting the heart is reduced.
Electrocardiogram: An electrocardiogram is a simple, painless test that measures the electrical activity of the heart.
Echocardiography: This test uses sound waves to produce live images of the heart to help your healthcare provider understand how your heart and its valves are functioning.
Bloodwork: Measures levels of certain cardiac enzymes. If cardiac enzymes are increased, this may indicate a problem with the heart.
Treatment
Treatment for intercostal neuralgia depends on the underlying cause and may include over-the-counter (OTC) and prescription medications and medical procedures.
OTC Medication
Over-the-counter (OTC) medication may help treat the pain associated with intercostal neuralgia. Some of these medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Infection with the varicella-zoster virus, the virus known for causing chickenpox and shingles
Participation in high speed or contact sports, such as skiing, snowboarding, football, and wrestling
Unsafe driving and automobile accidents, which may lead to injury to the intercostal nerves or ribs
Having a condition that causes systemic inflammation, such as inflammatory arthritis
Diagnosis
The majority of people with intercostal neuralgia first seek medical care because they think they may be having a heart attack or other cardiac problem.
The physical exam is an important part of the intercostal neuralgia diagnosis. It involves inspecting the area where the intercostal nerves are located. Pain produced from simple light pressure can help to assess the extent of pain.
To rule out other potential causes of chest wall pain, rib pain, or back pain, additional testing will be done. This will help your healthcare provider determine if the intercostal nerves are the source of pain or if there is another reason for your chest pain, such as lung or cardiovascular disease.
Other tests to help evaluate causes of pain related to the intercostal nerves include:
Chest X-ray: Can look for sources of chest, rib, and back pain and find problems in the airways, bones, heart, or lungs.
Nerve conduction velocity testing: Assesses nerve damage and dysfunction.
Electromyography: Evaluates the muscles and nerve cells that control them.
Musculoskeletal ultrasound: Involves more in-depth imaging than traditional X-rays or other imaging studies.
If you have risk factors for heart disease, such as diabetes, high blood pressure, a history of smoking, or a family history of heart disease, your healthcare provider will want to test your heart function.
Testing may include:
Exercise stress testing: Sometimes called a treadmill test, this test helps your healthcare provider figure out how much the heart can handle with exertion. As the body works harder, it needs more oxygen so it must pump more blood. The stress test can show if the blood supply to the arteries supporting the heart is reduced.
Electrocardiogram: An electrocardiogram is a simple, painless test that measures the electrical activity of the heart.
Echocardiography: This test uses sound waves to produce live images of the heart to help your healthcare provider understand how your heart and its valves are functioning.
Bloodwork: Measures levels of certain cardiac enzymes. If cardiac enzymes are increased, this may indicate a problem with the heart.
Treatment
Treatment for intercostal neuralgia depends on the underlying cause and may include over-the-counter (OTC) and prescription medications and medical procedures.
OTC Medication
Over-the-counter (OTC) medication may help treat the pain associated with intercostal neuralgia. Some of these medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
There are a number of risk factors that increase the chance of developing intercostal neuralgia.
Risk factors include:
Infection with the varicella-zoster virus, the virus known for causing chickenpox and shingles
Participation in high speed or contact sports, such as skiing, snowboarding, football, and wrestling
Unsafe driving and automobile accidents, which may lead to injury to the intercostal nerves or ribs
Having a condition that causes systemic inflammation, such as inflammatory arthritis
Diagnosis
The majority of people with intercostal neuralgia first seek medical care because they think they may be having a heart attack or other cardiac problem.
The physical exam is an important part of the intercostal neuralgia diagnosis. It involves inspecting the area where the intercostal nerves are located. Pain produced from simple light pressure can help to assess the extent of pain.
To rule out other potential causes of chest wall pain, rib pain, or back pain, additional testing will be done. This will help your healthcare provider determine if the intercostal nerves are the source of pain or if there is another reason for your chest pain, such as lung or cardiovascular disease.
Other tests to help evaluate causes of pain related to the intercostal nerves include:
Chest X-ray: Can look for sources of chest, rib, and back pain and find problems in the airways, bones, heart, or lungs.
Nerve conduction velocity testing: Assesses nerve damage and dysfunction.
Electromyography: Evaluates the muscles and nerve cells that control them.
Musculoskeletal ultrasound: Involves more in-depth imaging than traditional X-rays or other imaging studies.
If you have risk factors for heart disease, such as diabetes, high blood pressure, a history of smoking, or a family history of heart disease, your healthcare provider will want to test your heart function.
Testing may include:
Exercise stress testing: Sometimes called a treadmill test, this test helps your healthcare provider figure out how much the heart can handle with exertion. As the body works harder, it needs more oxygen so it must pump more blood. The stress test can show if the blood supply to the arteries supporting the heart is reduced.
Electrocardiogram: An electrocardiogram is a simple, painless test that measures the electrical activity of the heart.
Echocardiography: This test uses sound waves to produce live images of the heart to help your healthcare provider understand how your heart and its valves are functioning.
Bloodwork: Measures levels of certain cardiac enzymes. If cardiac enzymes are increased, this may indicate a problem with the heart.
Treatment
Treatment for intercostal neuralgia depends on the underlying cause and may include over-the-counter (OTC) and prescription medications and medical procedures.
OTC Medication
Over-the-counter (OTC) medication may help treat the pain associated with intercostal neuralgia. Some of these medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Chest trauma or muscle injury. Chest trauma such as a broken rib or bruised chest can cause intercostal neuralgia. You may also experience this type of pain if you pull or strain a muscle in the chest wall, shoulders, or back.
The shingles virus. A shingles infection can cause a type of intercostal neuralgia known as postherpetic neuralgia. People with this shingles complication may experience pain in the part of the body where shingles symptoms appeared. The pain may last for longer than 3 months and can continue even after the rash has disappeared. Postherpetic neuralgia can also cause extreme sensitivity to touch or temperature resulting in a burning sensation on the skin.
Intercostal nerve entrapment. This is when the intercostal nerve is compressed between other structures in the body such as a ligament and a bone. When these structures rub against the nerve, they can cause permanent damage leading to neuropathy symptoms.
Neuritis. An inflammation of the intercostal nerves can happen as a result of injury or infection. It may also have no known cause.
Post-thoracotomy pain syndrome (PTPS). This is a complication of a surgical procedure that involves opening the chest to access the throat, lungs, heart, or diaphragm.
A tumor. A tumor in the chest or abdomen can press on the intercostal nerves. These tumors can be benign (not cancer) or cancerous.
Pregnancy. Intercostal neuralgia can sometimes develop during pregnancy, though this is not common. Research suggests that this might happen as the growing uterus puts pressure on intercostal nerves.10 In most cases, the condition goes away after delivery.
Sometimes, intercostal neuralgia has no known cause. If your healthcare provider is unable to determine a cause, you may be diagnosed with idiopathic intercostal neuralgia. The term “idiopathic” is used to describe medical conditions that have no identifiable or clear cause.
Risk Factors
There are a number of risk factors that increase the chance of developing intercostal neuralgia.
Risk factors include:
Infection with the varicella-zoster virus, the virus known for causing chickenpox and shingles
Participation in high speed or contact sports, such as skiing, snowboarding, football, and wrestling
Unsafe driving and automobile accidents, which may lead to injury to the intercostal nerves or ribs
Having a condition that causes systemic inflammation, such as inflammatory arthritis
Diagnosis
The majority of people with intercostal neuralgia first seek medical care because they think they may be having a heart attack or other cardiac problem.
The physical exam is an important part of the intercostal neuralgia diagnosis. It involves inspecting the area where the intercostal nerves are located. Pain produced from simple light pressure can help to assess the extent of pain.
To rule out other potential causes of chest wall pain, rib pain, or back pain, additional testing will be done. This will help your healthcare provider determine if the intercostal nerves are the source of pain or if there is another reason for your chest pain, such as lung or cardiovascular disease.
Other tests to help evaluate causes of pain related to the intercostal nerves include:
Chest X-ray: Can look for sources of chest, rib, and back pain and find problems in the airways, bones, heart, or lungs.
Nerve conduction velocity testing: Assesses nerve damage and dysfunction.
Electromyography: Evaluates the muscles and nerve cells that control them.
Musculoskeletal ultrasound: Involves more in-depth imaging than traditional X-rays or other imaging studies.
If you have risk factors for heart disease, such as diabetes, high blood pressure, a history of smoking, or a family history of heart disease, your healthcare provider will want to test your heart function.
Testing may include:
Exercise stress testing: Sometimes called a treadmill test, this test helps your healthcare provider figure out how much the heart can handle with exertion. As the body works harder, it needs more oxygen so it must pump more blood. The stress test can show if the blood supply to the arteries supporting the heart is reduced.
Electrocardiogram: An electrocardiogram is a simple, painless test that measures the electrical activity of the heart.
Echocardiography: This test uses sound waves to produce live images of the heart to help your healthcare provider understand how your heart and its valves are functioning.
Bloodwork: Measures levels of certain cardiac enzymes. If cardiac enzymes are increased, this may indicate a problem with the heart.
Treatment
Treatment for intercostal neuralgia depends on the underlying cause and may include over-the-counter (OTC) and prescription medications and medical procedures.
OTC Medication
Over-the-counter (OTC) medication may help treat the pain associated with intercostal neuralgia. Some of these medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Chest or rib pain that spreads into the left arm, jaw, shoulder, or back
Chest pressure or tightening in the chest
Coughing up yellow-green colored mucus
Heart palpitations or a fluttering feeling in the chest
Breathing problems, such as shortness of breath or inability to take a full breath
Severe abdominal pain
Severe chest pain with breathing or coughing
Sudden confusion or dizziness, or changes in consciousness, such as passing out or unresponsiveness
Causes
Intercostal neuralgia is caused by inflammation and irritation in or compression of the intercostal nerves. Causes of intercostal nerve pain can vary from injury to the bones or muscles to a problem with the nerves.
Chest trauma or muscle injury. Chest trauma such as a broken rib or bruised chest can cause intercostal neuralgia. You may also experience this type of pain if you pull or strain a muscle in the chest wall, shoulders, or back.
The shingles virus. A shingles infection can cause a type of intercostal neuralgia known as postherpetic neuralgia. People with this shingles complication may experience pain in the part of the body where shingles symptoms appeared. The pain may last for longer than 3 months and can continue even after the rash has disappeared. Postherpetic neuralgia can also cause extreme sensitivity to touch or temperature resulting in a burning sensation on the skin.
Intercostal nerve entrapment. This is when the intercostal nerve is compressed between other structures in the body such as a ligament and a bone. When these structures rub against the nerve, they can cause permanent damage leading to neuropathy symptoms.
Neuritis. An inflammation of the intercostal nerves can happen as a result of injury or infection. It may also have no known cause.
Post-thoracotomy pain syndrome (PTPS). This is a complication of a surgical procedure that involves opening the chest to access the throat, lungs, heart, or diaphragm.
A tumor. A tumor in the chest or abdomen can press on the intercostal nerves. These tumors can be benign (not cancer) or cancerous.
Pregnancy. Intercostal neuralgia can sometimes develop during pregnancy, though this is not common. Research suggests that this might happen as the growing uterus puts pressure on intercostal nerves.10 In most cases, the condition goes away after delivery.
Sometimes, intercostal neuralgia has no known cause. If your healthcare provider is unable to determine a cause, you may be diagnosed with idiopathic intercostal neuralgia. The term “idiopathic” is used to describe medical conditions that have no identifiable or clear cause.
Risk Factors
There are a number of risk factors that increase the chance of developing intercostal neuralgia.
Risk factors include:
Infection with the varicella-zoster virus, the virus known for causing chickenpox and shingles
Participation in high speed or contact sports, such as skiing, snowboarding, football, and wrestling
Unsafe driving and automobile accidents, which may lead to injury to the intercostal nerves or ribs
Having a condition that causes systemic inflammation, such as inflammatory arthritis
Diagnosis
The majority of people with intercostal neuralgia first seek medical care because they think they may be having a heart attack or other cardiac problem.
The physical exam is an important part of the intercostal neuralgia diagnosis. It involves inspecting the area where the intercostal nerves are located. Pain produced from simple light pressure can help to assess the extent of pain.
To rule out other potential causes of chest wall pain, rib pain, or back pain, additional testing will be done. This will help your healthcare provider determine if the intercostal nerves are the source of pain or if there is another reason for your chest pain, such as lung or cardiovascular disease.
Other tests to help evaluate causes of pain related to the intercostal nerves include:
Chest X-ray: Can look for sources of chest, rib, and back pain and find problems in the airways, bones, heart, or lungs.
Nerve conduction velocity testing: Assesses nerve damage and dysfunction.
Electromyography: Evaluates the muscles and nerve cells that control them.
Musculoskeletal ultrasound: Involves more in-depth imaging than traditional X-rays or other imaging studies.
If you have risk factors for heart disease, such as diabetes, high blood pressure, a history of smoking, or a family history of heart disease, your healthcare provider will want to test your heart function.
Testing may include:
Exercise stress testing: Sometimes called a treadmill test, this test helps your healthcare provider figure out how much the heart can handle with exertion. As the body works harder, it needs more oxygen so it must pump more blood. The stress test can show if the blood supply to the arteries supporting the heart is reduced.
Electrocardiogram: An electrocardiogram is a simple, painless test that measures the electrical activity of the heart.
Echocardiography: This test uses sound waves to produce live images of the heart to help your healthcare provider understand how your heart and its valves are functioning.
Bloodwork: Measures levels of certain cardiac enzymes. If cardiac enzymes are increased, this may indicate a problem with the heart.
Treatment
Treatment for intercostal neuralgia depends on the underlying cause and may include over-the-counter (OTC) and prescription medications and medical procedures.
OTC Medication
Over-the-counter (OTC) medication may help treat the pain associated with intercostal neuralgia. Some of these medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
There are times when rib and chest pain may indicate a life-threatening condition. Intercostal neuralgia can cause severe and debilitating pain that makes it hard to breathe. Sometimes, rib cage pain or chest area pain can be a sign of a condition that may require emergency medical treatment. For example, chest pain may indicate a heart attack.
Other symptoms that may indicate a medical emergency include:
Chest or rib pain that spreads into the left arm, jaw, shoulder, or back
Chest pressure or tightening in the chest
Coughing up yellow-green colored mucus
Heart palpitations or a fluttering feeling in the chest
Breathing problems, such as shortness of breath or inability to take a full breath
Severe abdominal pain
Severe chest pain with breathing or coughing
Sudden confusion or dizziness, or changes in consciousness, such as passing out or unresponsiveness
Causes
Intercostal neuralgia is caused by inflammation and irritation in or compression of the intercostal nerves. Causes of intercostal nerve pain can vary from injury to the bones or muscles to a problem with the nerves.
Chest trauma or muscle injury. Chest trauma such as a broken rib or bruised chest can cause intercostal neuralgia. You may also experience this type of pain if you pull or strain a muscle in the chest wall, shoulders, or back.
The shingles virus. A shingles infection can cause a type of intercostal neuralgia known as postherpetic neuralgia. People with this shingles complication may experience pain in the part of the body where shingles symptoms appeared. The pain may last for longer than 3 months and can continue even after the rash has disappeared. Postherpetic neuralgia can also cause extreme sensitivity to touch or temperature resulting in a burning sensation on the skin.
Intercostal nerve entrapment. This is when the intercostal nerve is compressed between other structures in the body such as a ligament and a bone. When these structures rub against the nerve, they can cause permanent damage leading to neuropathy symptoms.
Neuritis. An inflammation of the intercostal nerves can happen as a result of injury or infection. It may also have no known cause.
Post-thoracotomy pain syndrome (PTPS). This is a complication of a surgical procedure that involves opening the chest to access the throat, lungs, heart, or diaphragm.
A tumor. A tumor in the chest or abdomen can press on the intercostal nerves. These tumors can be benign (not cancer) or cancerous.
Pregnancy. Intercostal neuralgia can sometimes develop during pregnancy, though this is not common. Research suggests that this might happen as the growing uterus puts pressure on intercostal nerves.10 In most cases, the condition goes away after delivery.
Sometimes, intercostal neuralgia has no known cause. If your healthcare provider is unable to determine a cause, you may be diagnosed with idiopathic intercostal neuralgia. The term “idiopathic” is used to describe medical conditions that have no identifiable or clear cause.
Risk Factors
There are a number of risk factors that increase the chance of developing intercostal neuralgia.
Risk factors include:
Infection with the varicella-zoster virus, the virus known for causing chickenpox and shingles
Participation in high speed or contact sports, such as skiing, snowboarding, football, and wrestling
Unsafe driving and automobile accidents, which may lead to injury to the intercostal nerves or ribs
Having a condition that causes systemic inflammation, such as inflammatory arthritis
Diagnosis
The majority of people with intercostal neuralgia first seek medical care because they think they may be having a heart attack or other cardiac problem.
The physical exam is an important part of the intercostal neuralgia diagnosis. It involves inspecting the area where the intercostal nerves are located. Pain produced from simple light pressure can help to assess the extent of pain.
To rule out other potential causes of chest wall pain, rib pain, or back pain, additional testing will be done. This will help your healthcare provider determine if the intercostal nerves are the source of pain or if there is another reason for your chest pain, such as lung or cardiovascular disease.
Other tests to help evaluate causes of pain related to the intercostal nerves include:
Chest X-ray: Can look for sources of chest, rib, and back pain and find problems in the airways, bones, heart, or lungs.
Nerve conduction velocity testing: Assesses nerve damage and dysfunction.
Electromyography: Evaluates the muscles and nerve cells that control them.
Musculoskeletal ultrasound: Involves more in-depth imaging than traditional X-rays or other imaging studies.
If you have risk factors for heart disease, such as diabetes, high blood pressure, a history of smoking, or a family history of heart disease, your healthcare provider will want to test your heart function.
Testing may include:
Exercise stress testing: Sometimes called a treadmill test, this test helps your healthcare provider figure out how much the heart can handle with exertion. As the body works harder, it needs more oxygen so it must pump more blood. The stress test can show if the blood supply to the arteries supporting the heart is reduced.
Electrocardiogram: An electrocardiogram is a simple, painless test that measures the electrical activity of the heart.
Echocardiography: This test uses sound waves to produce live images of the heart to help your healthcare provider understand how your heart and its valves are functioning.
Bloodwork: Measures levels of certain cardiac enzymes. If cardiac enzymes are increased, this may indicate a problem with the heart.
Treatment
Treatment for intercostal neuralgia depends on the underlying cause and may include over-the-counter (OTC) and prescription medications and medical procedures.
OTC Medication
Over-the-counter (OTC) medication may help treat the pain associated with intercostal neuralgia. Some of these medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
A squeezing sensation from the front of your chest to your back
Some people may also experience referred pain, which is related pain that appears in an unaffected part of the body. In people with intercostal neuralgia, the shoulder blade and lower pelvis are common sites for this type of pain.
When to Call Your Healthcare Provider
There are times when rib and chest pain may indicate a life-threatening condition. Intercostal neuralgia can cause severe and debilitating pain that makes it hard to breathe. Sometimes, rib cage pain or chest area pain can be a sign of a condition that may require emergency medical treatment. For example, chest pain may indicate a heart attack.
Other symptoms that may indicate a medical emergency include:
Chest or rib pain that spreads into the left arm, jaw, shoulder, or back
Chest pressure or tightening in the chest
Coughing up yellow-green colored mucus
Heart palpitations or a fluttering feeling in the chest
Breathing problems, such as shortness of breath or inability to take a full breath
Severe abdominal pain
Severe chest pain with breathing or coughing
Sudden confusion or dizziness, or changes in consciousness, such as passing out or unresponsiveness
Causes
Intercostal neuralgia is caused by inflammation and irritation in or compression of the intercostal nerves. Causes of intercostal nerve pain can vary from injury to the bones or muscles to a problem with the nerves.
Chest trauma or muscle injury. Chest trauma such as a broken rib or bruised chest can cause intercostal neuralgia. You may also experience this type of pain if you pull or strain a muscle in the chest wall, shoulders, or back.
The shingles virus. A shingles infection can cause a type of intercostal neuralgia known as postherpetic neuralgia. People with this shingles complication may experience pain in the part of the body where shingles symptoms appeared. The pain may last for longer than 3 months and can continue even after the rash has disappeared. Postherpetic neuralgia can also cause extreme sensitivity to touch or temperature resulting in a burning sensation on the skin.
Intercostal nerve entrapment. This is when the intercostal nerve is compressed between other structures in the body such as a ligament and a bone. When these structures rub against the nerve, they can cause permanent damage leading to neuropathy symptoms.
Neuritis. An inflammation of the intercostal nerves can happen as a result of injury or infection. It may also have no known cause.
Post-thoracotomy pain syndrome (PTPS). This is a complication of a surgical procedure that involves opening the chest to access the throat, lungs, heart, or diaphragm.
A tumor. A tumor in the chest or abdomen can press on the intercostal nerves. These tumors can be benign (not cancer) or cancerous.
Pregnancy. Intercostal neuralgia can sometimes develop during pregnancy, though this is not common. Research suggests that this might happen as the growing uterus puts pressure on intercostal nerves.10 In most cases, the condition goes away after delivery.
Sometimes, intercostal neuralgia has no known cause. If your healthcare provider is unable to determine a cause, you may be diagnosed with idiopathic intercostal neuralgia. The term “idiopathic” is used to describe medical conditions that have no identifiable or clear cause.
Risk Factors
There are a number of risk factors that increase the chance of developing intercostal neuralgia.
Risk factors include:
Infection with the varicella-zoster virus, the virus known for causing chickenpox and shingles
Participation in high speed or contact sports, such as skiing, snowboarding, football, and wrestling
Unsafe driving and automobile accidents, which may lead to injury to the intercostal nerves or ribs
Having a condition that causes systemic inflammation, such as inflammatory arthritis
Diagnosis
The majority of people with intercostal neuralgia first seek medical care because they think they may be having a heart attack or other cardiac problem.
The physical exam is an important part of the intercostal neuralgia diagnosis. It involves inspecting the area where the intercostal nerves are located. Pain produced from simple light pressure can help to assess the extent of pain.
To rule out other potential causes of chest wall pain, rib pain, or back pain, additional testing will be done. This will help your healthcare provider determine if the intercostal nerves are the source of pain or if there is another reason for your chest pain, such as lung or cardiovascular disease.
Other tests to help evaluate causes of pain related to the intercostal nerves include:
Chest X-ray: Can look for sources of chest, rib, and back pain and find problems in the airways, bones, heart, or lungs.
Nerve conduction velocity testing: Assesses nerve damage and dysfunction.
Electromyography: Evaluates the muscles and nerve cells that control them.
Musculoskeletal ultrasound: Involves more in-depth imaging than traditional X-rays or other imaging studies.
If you have risk factors for heart disease, such as diabetes, high blood pressure, a history of smoking, or a family history of heart disease, your healthcare provider will want to test your heart function.
Testing may include:
Exercise stress testing: Sometimes called a treadmill test, this test helps your healthcare provider figure out how much the heart can handle with exertion. As the body works harder, it needs more oxygen so it must pump more blood. The stress test can show if the blood supply to the arteries supporting the heart is reduced.
Electrocardiogram: An electrocardiogram is a simple, painless test that measures the electrical activity of the heart.
Echocardiography: This test uses sound waves to produce live images of the heart to help your healthcare provider understand how your heart and its valves are functioning.
Bloodwork: Measures levels of certain cardiac enzymes. If cardiac enzymes are increased, this may indicate a problem with the heart.
Treatment
Treatment for intercostal neuralgia depends on the underlying cause and may include over-the-counter (OTC) and prescription medications and medical procedures.
OTC Medication
Over-the-counter (OTC) medication may help treat the pain associated with intercostal neuralgia. Some of these medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Other symptoms of intercostal neuralgia may include:
Abdominal pain
Fever
Itchiness
Numbness
Tingling
Restricted mobility of shoulders and back
A squeezing sensation from the front of your chest to your back
Some people may also experience referred pain, which is related pain that appears in an unaffected part of the body. In people with intercostal neuralgia, the shoulder blade and lower pelvis are common sites for this type of pain.
When to Call Your Healthcare Provider
There are times when rib and chest pain may indicate a life-threatening condition. Intercostal neuralgia can cause severe and debilitating pain that makes it hard to breathe. Sometimes, rib cage pain or chest area pain can be a sign of a condition that may require emergency medical treatment. For example, chest pain may indicate a heart attack.
Other symptoms that may indicate a medical emergency include:
Chest or rib pain that spreads into the left arm, jaw, shoulder, or back
Chest pressure or tightening in the chest
Coughing up yellow-green colored mucus
Heart palpitations or a fluttering feeling in the chest
Breathing problems, such as shortness of breath or inability to take a full breath
Severe abdominal pain
Severe chest pain with breathing or coughing
Sudden confusion or dizziness, or changes in consciousness, such as passing out or unresponsiveness
Causes
Intercostal neuralgia is caused by inflammation and irritation in or compression of the intercostal nerves. Causes of intercostal nerve pain can vary from injury to the bones or muscles to a problem with the nerves.
Chest trauma or muscle injury. Chest trauma such as a broken rib or bruised chest can cause intercostal neuralgia. You may also experience this type of pain if you pull or strain a muscle in the chest wall, shoulders, or back.
The shingles virus. A shingles infection can cause a type of intercostal neuralgia known as postherpetic neuralgia. People with this shingles complication may experience pain in the part of the body where shingles symptoms appeared. The pain may last for longer than 3 months and can continue even after the rash has disappeared. Postherpetic neuralgia can also cause extreme sensitivity to touch or temperature resulting in a burning sensation on the skin.
Intercostal nerve entrapment. This is when the intercostal nerve is compressed between other structures in the body such as a ligament and a bone. When these structures rub against the nerve, they can cause permanent damage leading to neuropathy symptoms.
Neuritis. An inflammation of the intercostal nerves can happen as a result of injury or infection. It may also have no known cause.
Post-thoracotomy pain syndrome (PTPS). This is a complication of a surgical procedure that involves opening the chest to access the throat, lungs, heart, or diaphragm.
A tumor. A tumor in the chest or abdomen can press on the intercostal nerves. These tumors can be benign (not cancer) or cancerous.
Pregnancy. Intercostal neuralgia can sometimes develop during pregnancy, though this is not common. Research suggests that this might happen as the growing uterus puts pressure on intercostal nerves.10 In most cases, the condition goes away after delivery.
Sometimes, intercostal neuralgia has no known cause. If your healthcare provider is unable to determine a cause, you may be diagnosed with idiopathic intercostal neuralgia. The term “idiopathic” is used to describe medical conditions that have no identifiable or clear cause.
Risk Factors
There are a number of risk factors that increase the chance of developing intercostal neuralgia.
Risk factors include:
Infection with the varicella-zoster virus, the virus known for causing chickenpox and shingles
Participation in high speed or contact sports, such as skiing, snowboarding, football, and wrestling
Unsafe driving and automobile accidents, which may lead to injury to the intercostal nerves or ribs
Having a condition that causes systemic inflammation, such as inflammatory arthritis
Diagnosis
The majority of people with intercostal neuralgia first seek medical care because they think they may be having a heart attack or other cardiac problem.
The physical exam is an important part of the intercostal neuralgia diagnosis. It involves inspecting the area where the intercostal nerves are located. Pain produced from simple light pressure can help to assess the extent of pain.
To rule out other potential causes of chest wall pain, rib pain, or back pain, additional testing will be done. This will help your healthcare provider determine if the intercostal nerves are the source of pain or if there is another reason for your chest pain, such as lung or cardiovascular disease.
Other tests to help evaluate causes of pain related to the intercostal nerves include:
Chest X-ray: Can look for sources of chest, rib, and back pain and find problems in the airways, bones, heart, or lungs.
Nerve conduction velocity testing: Assesses nerve damage and dysfunction.
Electromyography: Evaluates the muscles and nerve cells that control them.
Musculoskeletal ultrasound: Involves more in-depth imaging than traditional X-rays or other imaging studies.
If you have risk factors for heart disease, such as diabetes, high blood pressure, a history of smoking, or a family history of heart disease, your healthcare provider will want to test your heart function.
Testing may include:
Exercise stress testing: Sometimes called a treadmill test, this test helps your healthcare provider figure out how much the heart can handle with exertion. As the body works harder, it needs more oxygen so it must pump more blood. The stress test can show if the blood supply to the arteries supporting the heart is reduced.
Electrocardiogram: An electrocardiogram is a simple, painless test that measures the electrical activity of the heart.
Echocardiography: This test uses sound waves to produce live images of the heart to help your healthcare provider understand how your heart and its valves are functioning.
Bloodwork: Measures levels of certain cardiac enzymes. If cardiac enzymes are increased, this may indicate a problem with the heart.
Treatment
Treatment for intercostal neuralgia depends on the underlying cause and may include over-the-counter (OTC) and prescription medications and medical procedures.
OTC Medication
Over-the-counter (OTC) medication may help treat the pain associated with intercostal neuralgia. Some of these medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
You may feel this pain around your ribs or in your upper chest or back. The pain might cover the entire chest or radiate from the back towards the chest. Sometimes the pain can be felt along the length of the ribs. Pain episodes tend to be sporadic and may intensify with activity, including:
Lifting
Turning and twisting the torso
Coughing
Sneezing
Laughing
Breathing deeply
Other symptoms of intercostal neuralgia may include:
Abdominal pain
Fever
Itchiness
Numbness
Tingling
Restricted mobility of shoulders and back
A squeezing sensation from the front of your chest to your back
Some people may also experience referred pain, which is related pain that appears in an unaffected part of the body. In people with intercostal neuralgia, the shoulder blade and lower pelvis are common sites for this type of pain.
When to Call Your Healthcare Provider
There are times when rib and chest pain may indicate a life-threatening condition. Intercostal neuralgia can cause severe and debilitating pain that makes it hard to breathe. Sometimes, rib cage pain or chest area pain can be a sign of a condition that may require emergency medical treatment. For example, chest pain may indicate a heart attack.
Other symptoms that may indicate a medical emergency include:
Chest or rib pain that spreads into the left arm, jaw, shoulder, or back
Chest pressure or tightening in the chest
Coughing up yellow-green colored mucus
Heart palpitations or a fluttering feeling in the chest
Breathing problems, such as shortness of breath or inability to take a full breath
Severe abdominal pain
Severe chest pain with breathing or coughing
Sudden confusion or dizziness, or changes in consciousness, such as passing out or unresponsiveness
Causes
Intercostal neuralgia is caused by inflammation and irritation in or compression of the intercostal nerves. Causes of intercostal nerve pain can vary from injury to the bones or muscles to a problem with the nerves.
Chest trauma or muscle injury. Chest trauma such as a broken rib or bruised chest can cause intercostal neuralgia. You may also experience this type of pain if you pull or strain a muscle in the chest wall, shoulders, or back.
The shingles virus. A shingles infection can cause a type of intercostal neuralgia known as postherpetic neuralgia. People with this shingles complication may experience pain in the part of the body where shingles symptoms appeared. The pain may last for longer than 3 months and can continue even after the rash has disappeared. Postherpetic neuralgia can also cause extreme sensitivity to touch or temperature resulting in a burning sensation on the skin.
Intercostal nerve entrapment. This is when the intercostal nerve is compressed between other structures in the body such as a ligament and a bone. When these structures rub against the nerve, they can cause permanent damage leading to neuropathy symptoms.
Neuritis. An inflammation of the intercostal nerves can happen as a result of injury or infection. It may also have no known cause.
Post-thoracotomy pain syndrome (PTPS). This is a complication of a surgical procedure that involves opening the chest to access the throat, lungs, heart, or diaphragm.
A tumor. A tumor in the chest or abdomen can press on the intercostal nerves. These tumors can be benign (not cancer) or cancerous.
Pregnancy. Intercostal neuralgia can sometimes develop during pregnancy, though this is not common. Research suggests that this might happen as the growing uterus puts pressure on intercostal nerves.10 In most cases, the condition goes away after delivery.
Sometimes, intercostal neuralgia has no known cause. If your healthcare provider is unable to determine a cause, you may be diagnosed with idiopathic intercostal neuralgia. The term “idiopathic” is used to describe medical conditions that have no identifiable or clear cause.
Risk Factors
There are a number of risk factors that increase the chance of developing intercostal neuralgia.
Risk factors include:
Infection with the varicella-zoster virus, the virus known for causing chickenpox and shingles
Participation in high speed or contact sports, such as skiing, snowboarding, football, and wrestling
Unsafe driving and automobile accidents, which may lead to injury to the intercostal nerves or ribs
Having a condition that causes systemic inflammation, such as inflammatory arthritis
Diagnosis
The majority of people with intercostal neuralgia first seek medical care because they think they may be having a heart attack or other cardiac problem.
The physical exam is an important part of the intercostal neuralgia diagnosis. It involves inspecting the area where the intercostal nerves are located. Pain produced from simple light pressure can help to assess the extent of pain.
To rule out other potential causes of chest wall pain, rib pain, or back pain, additional testing will be done. This will help your healthcare provider determine if the intercostal nerves are the source of pain or if there is another reason for your chest pain, such as lung or cardiovascular disease.
Other tests to help evaluate causes of pain related to the intercostal nerves include:
Chest X-ray: Can look for sources of chest, rib, and back pain and find problems in the airways, bones, heart, or lungs.
Nerve conduction velocity testing: Assesses nerve damage and dysfunction.
Electromyography: Evaluates the muscles and nerve cells that control them.
Musculoskeletal ultrasound: Involves more in-depth imaging than traditional X-rays or other imaging studies.
If you have risk factors for heart disease, such as diabetes, high blood pressure, a history of smoking, or a family history of heart disease, your healthcare provider will want to test your heart function.
Testing may include:
Exercise stress testing: Sometimes called a treadmill test, this test helps your healthcare provider figure out how much the heart can handle with exertion. As the body works harder, it needs more oxygen so it must pump more blood. The stress test can show if the blood supply to the arteries supporting the heart is reduced.
Electrocardiogram: An electrocardiogram is a simple, painless test that measures the electrical activity of the heart.
Echocardiography: This test uses sound waves to produce live images of the heart to help your healthcare provider understand how your heart and its valves are functioning.
Bloodwork: Measures levels of certain cardiac enzymes. If cardiac enzymes are increased, this may indicate a problem with the heart.
Treatment
Treatment for intercostal neuralgia depends on the underlying cause and may include over-the-counter (OTC) and prescription medications and medical procedures.
OTC Medication
Over-the-counter (OTC) medication may help treat the pain associated with intercostal neuralgia. Some of these medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
The main symptom experienced by people with intercostal neuralgia is pain in the rib cage area. People who experience this type of rib pain may describe the pain as:
Stabbing
Sharp
Tender
Aching
Gnawing
Burning
Spasm-like
You may feel this pain around your ribs or in your upper chest or back. The pain might cover the entire chest or radiate from the back towards the chest. Sometimes the pain can be felt along the length of the ribs. Pain episodes tend to be sporadic and may intensify with activity, including:
Lifting
Turning and twisting the torso
Coughing
Sneezing
Laughing
Breathing deeply
Other symptoms of intercostal neuralgia may include:
Abdominal pain
Fever
Itchiness
Numbness
Tingling
Restricted mobility of shoulders and back
A squeezing sensation from the front of your chest to your back
Some people may also experience referred pain, which is related pain that appears in an unaffected part of the body. In people with intercostal neuralgia, the shoulder blade and lower pelvis are common sites for this type of pain.
When to Call Your Healthcare Provider
There are times when rib and chest pain may indicate a life-threatening condition. Intercostal neuralgia can cause severe and debilitating pain that makes it hard to breathe. Sometimes, rib cage pain or chest area pain can be a sign of a condition that may require emergency medical treatment. For example, chest pain may indicate a heart attack.
Other symptoms that may indicate a medical emergency include:
Chest or rib pain that spreads into the left arm, jaw, shoulder, or back
Chest pressure or tightening in the chest
Coughing up yellow-green colored mucus
Heart palpitations or a fluttering feeling in the chest
Breathing problems, such as shortness of breath or inability to take a full breath
Severe abdominal pain
Severe chest pain with breathing or coughing
Sudden confusion or dizziness, or changes in consciousness, such as passing out or unresponsiveness
Causes
Intercostal neuralgia is caused by inflammation and irritation in or compression of the intercostal nerves. Causes of intercostal nerve pain can vary from injury to the bones or muscles to a problem with the nerves.
Chest trauma or muscle injury. Chest trauma such as a broken rib or bruised chest can cause intercostal neuralgia. You may also experience this type of pain if you pull or strain a muscle in the chest wall, shoulders, or back.
The shingles virus. A shingles infection can cause a type of intercostal neuralgia known as postherpetic neuralgia. People with this shingles complication may experience pain in the part of the body where shingles symptoms appeared. The pain may last for longer than 3 months and can continue even after the rash has disappeared. Postherpetic neuralgia can also cause extreme sensitivity to touch or temperature resulting in a burning sensation on the skin.
Intercostal nerve entrapment. This is when the intercostal nerve is compressed between other structures in the body such as a ligament and a bone. When these structures rub against the nerve, they can cause permanent damage leading to neuropathy symptoms.
Neuritis. An inflammation of the intercostal nerves can happen as a result of injury or infection. It may also have no known cause.
Post-thoracotomy pain syndrome (PTPS). This is a complication of a surgical procedure that involves opening the chest to access the throat, lungs, heart, or diaphragm.
A tumor. A tumor in the chest or abdomen can press on the intercostal nerves. These tumors can be benign (not cancer) or cancerous.
Pregnancy. Intercostal neuralgia can sometimes develop during pregnancy, though this is not common. Research suggests that this might happen as the growing uterus puts pressure on intercostal nerves.10 In most cases, the condition goes away after delivery.
Sometimes, intercostal neuralgia has no known cause. If your healthcare provider is unable to determine a cause, you may be diagnosed with idiopathic intercostal neuralgia. The term “idiopathic” is used to describe medical conditions that have no identifiable or clear cause.
Risk Factors
There are a number of risk factors that increase the chance of developing intercostal neuralgia.
Risk factors include:
Infection with the varicella-zoster virus, the virus known for causing chickenpox and shingles
Participation in high speed or contact sports, such as skiing, snowboarding, football, and wrestling
Unsafe driving and automobile accidents, which may lead to injury to the intercostal nerves or ribs
Having a condition that causes systemic inflammation, such as inflammatory arthritis
Diagnosis
The majority of people with intercostal neuralgia first seek medical care because they think they may be having a heart attack or other cardiac problem.
The physical exam is an important part of the intercostal neuralgia diagnosis. It involves inspecting the area where the intercostal nerves are located. Pain produced from simple light pressure can help to assess the extent of pain.
To rule out other potential causes of chest wall pain, rib pain, or back pain, additional testing will be done. This will help your healthcare provider determine if the intercostal nerves are the source of pain or if there is another reason for your chest pain, such as lung or cardiovascular disease.
Other tests to help evaluate causes of pain related to the intercostal nerves include:
Chest X-ray: Can look for sources of chest, rib, and back pain and find problems in the airways, bones, heart, or lungs.
Nerve conduction velocity testing: Assesses nerve damage and dysfunction.
Electromyography: Evaluates the muscles and nerve cells that control them.
Musculoskeletal ultrasound: Involves more in-depth imaging than traditional X-rays or other imaging studies.
If you have risk factors for heart disease, such as diabetes, high blood pressure, a history of smoking, or a family history of heart disease, your healthcare provider will want to test your heart function.
Testing may include:
Exercise stress testing: Sometimes called a treadmill test, this test helps your healthcare provider figure out how much the heart can handle with exertion. As the body works harder, it needs more oxygen so it must pump more blood. The stress test can show if the blood supply to the arteries supporting the heart is reduced.
Electrocardiogram: An electrocardiogram is a simple, painless test that measures the electrical activity of the heart.
Echocardiography: This test uses sound waves to produce live images of the heart to help your healthcare provider understand how your heart and its valves are functioning.
Bloodwork: Measures levels of certain cardiac enzymes. If cardiac enzymes are increased, this may indicate a problem with the heart.
Treatment
Treatment for intercostal neuralgia depends on the underlying cause and may include over-the-counter (OTC) and prescription medications and medical procedures.
OTC Medication
Over-the-counter (OTC) medication may help treat the pain associated with intercostal neuralgia. Some of these medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs): NSAID pain relievers, such as Advil (ibuprofen) and Aleve (naproxen), can help reduce inflammation and pain.
Capsaicin cream: Can help with pain relief.
Prescription Medication
f OTC medication doesn’t help, talk to your healthcare provider about prescription medications such as:
Anti-depressants: Tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors may be helpful for reducing and treating nerve pain.
Anticonvulsants: Medications such as Neurontin (gabapentin), Tegretol (carbamazepine), and Lyrica (pregabalin) interfere with the transmission of pain signals in the body.
Opioids: If your pain is severe, your healthcare provider may prescribe opioid medication to help relieve your symptoms.
Procedures
Certain medical procedures can also help treat intercostal neuralgia. These procedures involve blocking or destroying the nerves that are causing the pain:
Intercostal nerve blocks: Injections of either a local anesthetic or a corticosteroid given around the affected intercostal nerves.
Radiofrequency ablation: This treatment is usually offered to people who experience frequent episodes of intercostal nerve pain. It involves destroying the specific part of the nerve that is causing pain and other symptoms of intercostal neuralgia.
Complementary Therapies
Your healthcare provider may also recommend complementary therapies, such as:
Acupuncture: This traditional Chinese medicine practice involves inserting fine needles into certain points on the body to relieve pain.
Massage therapy: Massaging the related muscles, ligaments, and tendons may help relieve some of your pain.
Yoga: Yoga and gentle stretching may help relieve pain. Try standing tall and raising your arms above your head. Clasp your hands together and then slowly lean to the right, then to the left. Hold the stretch for a few seconds on each side, or as long as is comfortable.
Transcutaneous electrical nerve stimulation (TENS): A TENS device delivers a low-voltage electrical current to the affected part of the body.
These therapies are to be used in conjunction with traditional treatments, and not as lone therapies or as substitutes for medicinal therapies.
Does Intercostal Neuralgia Go Away?
Depending on the cause, intercostal neuralgia may go away in a few weeks to months with treatment. It is also possible for symptoms to resolve on their own without treatment. Some people, however, will continue to experience chronic pain for the long term.
If your pain is caused by PTPS, for example, you may still experience mild neuralgia symptoms for years after your surgery.
Intercostal pain from a shingles infection can last for months or even years after the rash goes away. If you develop shingles, taking antiviral medication within 72 hours of the rash’s appearance can help prevent postherpetic neuralgia.
Prevention
Some healthy lifestyle habits may prevent intercostal neuralgia and reduce your risk of developing the condition.
Things you can do to reduce your risk are:
Driving motor vehicles safely and wearing a seatbelt
Getting vaccinated for chickenpox
Getting vaccinated for herpes or shingles if you are age 50 and older22
Wearing protective sports equipment, including helmets and padding
Working with your healthcare provider to manage symptoms of an inflammatory disease
Summary
Intercostal neuralgia is a type of nerve pain that’s felt in the chest. It occurs when the intercostal nerves are inflamed, irritated, or compressed. The pain can have a number of possible causes, including chest trauma, shingles, or a pulled or strained muscle.
Intercostal neuralgia can sometimes be mistaken for a heart attack. If you’re experiencing this kind of pain, your healthcare provider may want to test your heart function before diagnosing you.
Treatment for intercostal neuralgia may include pain medications, nerve blocks, anti-depressants, and more. It can often be prevented with safety precautions and getting a shingles vaccine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Exercise prescription for shoulder related injuries are specific to the case, as determined by the examination and evaluation of your treating therapist. While many exercises may help relieve pain, improve flexibility, or improve strength, the exercises that are prescribed to you are specific to your pathology.Exercise prescription for shoulder related injuries may reflect some general principles in regards to mob. However, Sports specific demands based on your activity level, including competition will drive the strength training portion of a sport specific rehab program.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Length of program: This shoulder conditioning program should be continued for 4 to 6 weeks, unless otherwise specified by your doctor or physical therapist. After your recovery, these exercises can be continued as a maintenance program for lifelong protection and health of your shoulders. Performing the exercises 2 to 3 days a week will maintain strength and range of motion in your shoulders.
Exercise prescription for shoulder related injuries are specific to the case, as determined by the examination and evaluation of your treating therapist. While many exercises may help relieve pain, improve flexibility, or improve strength, the exercises that are prescribed to you are specific to your pathology.Exercise prescription for shoulder related injuries may reflect some general principles in regards to mob. However, Sports specific demands based on your activity level, including competition will drive the strength training portion of a sport specific rehab program.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Length of program: This shoulder conditioning program should be continued for 4 to 6 weeks, unless otherwise specified by your doctor or physical therapist. After your recovery, these exercises can be continued as a maintenance program for lifelong protection and health of your shoulders. Performing the exercises 2 to 3 days a week will maintain strength and range of motion in your shoulders.
Exercise prescription for shoulder related injuries are specific to the case, as determined by the examination and evaluation of your treating therapist. While many exercises may help relieve pain, improve flexibility, or improve strength, the exercises that are prescribed to you are specific to your pathology.Exercise prescription for shoulder related injuries may reflect some general principles in regards to mob. However, Sports specific demands based on your activity level, including competition will drive the strength training portion of a sport specific rehab program.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following a well-structured conditioning program will also help you return to sports and other recreational activities.
This is a general conditioning program that provides a wide range of exercises. To ensure that the program is safe and effective for you, it should be performed under your doctor’s supervision. Talk to your doctor or physical therapist about which exercises will best help you meet your rehabilitation goals.
Strength: Strengthening the muscles that support your shoulder will help keep your shoulder joint stable. Keeping these muscles strong can relieve shoulder pain and prevent further injury.
Flexibility: Stretching the muscles that you strengthen is important for restoring range of motion and preventing injury. Gently stretching after strengthening exercises can help reduce muscle soreness and keep your muscles long and flexible.
Target Muscles: The muscle groups targeted in this conditioning program include:
Deltoids (front, back and over the shoulder)
Trapezius muscles (upper back)
Rhomboid muscles (upper back)
Teres muscles (supporting the shoulder joint)
Supraspinatus (supporting the shoulder joint)
Infraspinatus (supporting the shoulder joint)
Subscapularis (front of shoulder)
Biceps (front of upper arm)
Triceps (back of upper arm)
Length of program: This shoulder conditioning program should be continued for 4 to 6 weeks, unless otherwise specified by your doctor or physical therapist. After your recovery, these exercises can be continued as a maintenance program for lifelong protection and health of your shoulders. Performing the exercises 2 to 3 days a week will maintain strength and range of motion in your shoulders.
Exercise prescription for shoulder related injuries are specific to the case, as determined by the examination and evaluation of your treating therapist. While many exercises may help relieve pain, improve flexibility, or improve strength, the exercises that are prescribed to you are specific to your pathology.Exercise prescription for shoulder related injuries may reflect some general principles in regards to mob. However, Sports specific demands based on your activity level, including competition will drive the strength training portion of a sport specific rehab program.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Your shoulder is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle). The shoulder is a ball-and-socket joint: The ball, or head, of your upper arm bone fits into a shallow socket in your shoulder blade.
Your arm is kept in your shoulder socket by your rotator cuff. The rotator cuff is a network of four muscles that come together as tendonsto form a covering around the head of the humerus. The rotator cuff attaches the humerus to the shoulder blade and helps to lift and rotate your arm.
There is a lubricating sac called a bursa between the rotator cuff and the bone on top of your shoulder (acromion). The bursa allows the rotator cuff tendons to glide freely when you move your arm. When the rotator cuff tendons are injured or damaged, this bursa can also become inflamed and painful.
How will I know if I have a cuff tear?
In many cases, torn tendons begin by fraying (partial tears or intra-substance). As the damage progresses, the tendon can completely tear, sometimes with lifting a heavy object.
When one or more of the rotator cuff tendons is torn, the tendon no longer fully attaches to the head of the humerus. Most tears occur in the supraspinatus muscle and tendon, but other parts of the rotator cuff may also be involved.
Typically, you will feel pain in the front of your shoulder that radiates down the side of your arm. It may be present with overhead activities such as lifting or reaching. You may feel pain when you try to sleep on the affected side. You may note weakness of your arm and difficulty with routine activities such as combing your hair or reaching behind your back.
If the tear occurs with injury, you may experience acute pain, a snapping sensation, and immediate weakness of the arm. These symptoms can occur more easily after injury in an ageing patient.
What symptoms should I look out for?
The signs and symptoms of a rotator cuff tear depend on the size and extent of the tear and the length of time that it has been present. In most cases, pain is the predominant feature. This occurs because of inflammation around the damaged tendon, as well as mechanical catching of the tendon in its tunnel under the acromion. The pain occurs with use of the arm, particularly elevation to and above shoulder height. Pain also occurs at night, which is particularly disabling because of the interference with sleep. Weakness, associated loss of power and movement may occur, depending on the size of the tear.
Once the rotator cuff tears, it does not heal, and surgery may be necessary to repair the tendon. If extensive tears are not treated, the result is deteriorating shoulder function, the onset of widespread arthritis in the shoulder region, and increasing pain over time. The ability to offer surgery to repair torn tendons depends on many factors and unfortunately not all patients are candidates for successful surgery.
The most common symptoms of a rotator cuff tear include:
Pain at rest and at night, particularly if lying on the affected shoulder
Pain when lifting and lowering your arm or with specific movements
Weakness when lifting or rotating your arm
Crepitus or crackling sensation when moving your shoulder in certain positions
Tears that develop slowly due to overuse also cause pain and may cause arm weakness. You may have pain in the shoulder when you lift your arm to the side, or pain that moves down your arm. At first, the pain may be mild and only present when lifting your arm over your head, such as reaching into a cupboard. Over-the-counter medication, such as aspirin or ibuprofen, may initially relieve the pain.
Over time, the pain may become more noticeable at rest, and no longer goes away with medications. You may have pain when you lie on the painful side at night. The pain and weakness in the shoulder may make routine activities such as combing your hair or reaching behind your back more difficult.
There are different types of tears:
Partial Tear – (Intra-articular/bursal surface/intra-substance) This type of tear damages the soft tissue, but does not completely sever the tendon.
Full-Thickness Tear – This type of tear is also called a complete tear. It splits the soft tissue into two pieces. In many cases, tendons tear off where they attach to the head of the humerus. With a full-thickness tear, there is basically a hole in the tendon.
If I have a painful rotator cuff and keep using it, will this cause further damage?
A rotator cuff tear can extend or get larger over time. This can occur with repetitive use or a re-injury. It is common for patients with known rotator cuff disease to have acute pain and weakness following a minor injury. This likely represents extension of an existing tear.If you know you have a rotator cuff tear, then worsening pain and decreasing strength may mean the tear is getting larger.
Early diagnosis and treatment of a rotator cuff tear may prevent symptoms such as loss of strength and loss of motion from setting in. A consultation with an orthopaedic surgeon is recommended, and an Ultrasound/MRI is usually required to confirm the diagnosis. Appropriate surgical or non-surgical treatment can then begin.
What treatment options are available?
The goal of any treatment is to reduce pain and restore function. There are several treatment options for a rotator cuff tear, and the best option is different for each person. In planning your treatment, your doctor will consider your age, activity level, general health, and the type of tear that you have.
Surgical treatment is not necessary if pain and loss of function are not significant problems depending on your age and the circumstances of how the tear occurred. Non-operative treatment includes analgesics such as paracetamol and/or anti-inflammatories, and physiotherapy to strengthen the rotator cuff muscles provided it does not aggravating the problem. Particularly useful in the early stages are steroid injections but their benefit usually reduces with repeated injections. Injections should be administered under USS guidance to increase their accuracy.
Surgery is recommended if you have persistent pain or weakness and loss of function that does not improve with nonsurgical treatment. Frequently, patients who require surgery will report pain at night and difficulty using the arm for lifting and reaching. Many will report ongoing symptoms despite several months of medication and limited use of the arm.
Non-surgical treatment options may include:
Rest – Your doctor may suggest rest and limiting overhead activities.
Activity modification – Avoid activities that cause shoulder pain.
Non-steroidal anti-inflammatory medication – Drugs like ibuprofen reduce pain and swelling.
Strengthening exercises and physiotherapy – Specific exercises will restore movement and strengthen your shoulder. Your exercise program will include stretches to improve flexibility and range of motion. Strengthening the muscles that support your shoulder can relieve pain and prevent further injury.
Steroid injection – If rest, medications, and physiotherapy do not relieve your pain, an injection of a local anaesthetic and a cortisone preparation may be helpful. Cortisone is a very effective anti-inflammatory medicine.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
For the vast majority of people a scan is unnecessary. For most cases of lower back pain, a comprehensive physiotherapy assessment provides all the information we need to treat your pain effectively.
Imaging of the lower back can sometimes be confusing. We know that many abnormalities seen on scans do not actually cause symptoms, and many people without lower back pain will have similar ‘abnormalities’. One large scientific study found that 50% of people over the age of 30 WITHOUT back pain had disc problems! And that prevalence increased with age. If we treated everyone based solely on what was evident on the scan, the real problem could be missed and hence would not improve. In cases where our examination indicates a serious pathology, we will refer you for a scan and/or to a specialist for further examination.
How can physiotherapy help my lower back pain?
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Radicular referred pain is the term used to describe symptoms in the leg that are due to compression or irritation of a nerve root in the lower back. The nerve root may be physically obstructed by a disc, bone or ligament in the spine, or may be irritated by the inflammatory chemicals that are associated with an injury to one of these structures. Pain in the leg will often follow a “dermatomal” pattern, where the symptoms travel in a line from the lower back down to the foot. There may also be numbness of the skin or weakness of the muscles that are supplied by affected nerve root. It is essential that radicular referral pain is assessed thoroughly by a trained professional such as a physiotherapist, as these nerve injuries can lead to weakness that can be longstanding.
Should I get a scan for my lower back pain?
For the vast majority of people a scan is unnecessary. For most cases of lower back pain, a comprehensive physiotherapy assessment provides all the information we need to treat your pain effectively.
Imaging of the lower back can sometimes be confusing. We know that many abnormalities seen on scans do not actually cause symptoms, and many people without lower back pain will have similar ‘abnormalities’. One large scientific study found that 50% of people over the age of 30 WITHOUT back pain had disc problems! And that prevalence increased with age. If we treated everyone based solely on what was evident on the scan, the real problem could be missed and hence would not improve. In cases where our examination indicates a serious pathology, we will refer you for a scan and/or to a specialist for further examination.
How can physiotherapy help my lower back pain?
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Somatic referred pain is the most common cause of leg symptoms in patients with lower back pain and is often the cause of pain in the buttock or back of the thigh. The symptoms are due to referred pain, where the pain sensations from the lower back are mixed with the sensations from the leg. In this case there is no direct compression or irritation of the nerve roots that exit the spine, it is simply due to “cross-talk” between the sensory nerves coming from the muscles/joints of the back and those coming from the muscles/skin of the legs. This phenomenon occurs in many other areas of the body, such as shoulder symptoms with neck pain or thigh/knee symptoms with hip pain. Somatic referred pain is not associated with any loss of sensation or weakness in the legs.
Radicular referred pain is the term used to describe symptoms in the leg that are due to compression or irritation of a nerve root in the lower back. The nerve root may be physically obstructed by a disc, bone or ligament in the spine, or may be irritated by the inflammatory chemicals that are associated with an injury to one of these structures. Pain in the leg will often follow a “dermatomal” pattern, where the symptoms travel in a line from the lower back down to the foot. There may also be numbness of the skin or weakness of the muscles that are supplied by affected nerve root. It is essential that radicular referral pain is assessed thoroughly by a trained professional such as a physiotherapist, as these nerve injuries can lead to weakness that can be longstanding.
Should I get a scan for my lower back pain?
For the vast majority of people a scan is unnecessary. For most cases of lower back pain, a comprehensive physiotherapy assessment provides all the information we need to treat your pain effectively.
Imaging of the lower back can sometimes be confusing. We know that many abnormalities seen on scans do not actually cause symptoms, and many people without lower back pain will have similar ‘abnormalities’. One large scientific study found that 50% of people over the age of 30 WITHOUT back pain had disc problems! And that prevalence increased with age. If we treated everyone based solely on what was evident on the scan, the real problem could be missed and hence would not improve. In cases where our examination indicates a serious pathology, we will refer you for a scan and/or to a specialist for further examination.
How can physiotherapy help my lower back pain?
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
I also have pain in my buttock or running down my leg from my back. What does that mean?
Leg symptoms associated with lower back pain, often referred to as “sciatica”, can be due to either somatic referred pain or radicular referred pain, both of which are described below. Physiotherapists are trained to use specific tests to determine the cause of leg symptoms and treat them appropriately.
Somatic referred pain is the most common cause of leg symptoms in patients with lower back pain and is often the cause of pain in the buttock or back of the thigh. The symptoms are due to referred pain, where the pain sensations from the lower back are mixed with the sensations from the leg. In this case there is no direct compression or irritation of the nerve roots that exit the spine, it is simply due to “cross-talk” between the sensory nerves coming from the muscles/joints of the back and those coming from the muscles/skin of the legs. This phenomenon occurs in many other areas of the body, such as shoulder symptoms with neck pain or thigh/knee symptoms with hip pain. Somatic referred pain is not associated with any loss of sensation or weakness in the legs.
Radicular referred pain is the term used to describe symptoms in the leg that are due to compression or irritation of a nerve root in the lower back. The nerve root may be physically obstructed by a disc, bone or ligament in the spine, or may be irritated by the inflammatory chemicals that are associated with an injury to one of these structures. Pain in the leg will often follow a “dermatomal” pattern, where the symptoms travel in a line from the lower back down to the foot. There may also be numbness of the skin or weakness of the muscles that are supplied by affected nerve root. It is essential that radicular referral pain is assessed thoroughly by a trained professional such as a physiotherapist, as these nerve injuries can lead to weakness that can be longstanding.
Should I get a scan for my lower back pain?
For the vast majority of people a scan is unnecessary. For most cases of lower back pain, a comprehensive physiotherapy assessment provides all the information we need to treat your pain effectively.
Imaging of the lower back can sometimes be confusing. We know that many abnormalities seen on scans do not actually cause symptoms, and many people without lower back pain will have similar ‘abnormalities’. One large scientific study found that 50% of people over the age of 30 WITHOUT back pain had disc problems! And that prevalence increased with age. If we treated everyone based solely on what was evident on the scan, the real problem could be missed and hence would not improve. In cases where our examination indicates a serious pathology, we will refer you for a scan and/or to a specialist for further examination.
How can physiotherapy help my lower back pain?
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
In many cases of lower back pain, it is difficult to identify exactly which structure is causing the pain. During our examination, the first step will be to rule out anything serious.
We will test the spine’s function and decide where there are restrictions in movement or muscle contraction. Back pain is usually caused by a combination of structures and movement patterns rather than one specific joint, disc or muscle. Therefore, trying to pinpoint one specific structure as the cause of the symptoms is often misleading. We base our treatment both on the presenting symptoms as well as movement and activation patterns of the back. We aim to improve function, leading to an immediate reduction in pain and restore normal pain-free movement. There are other factors that are frequently associated with lower back pain, particularly when a person has longstanding or recurrent symptoms.
These may include poor sleep quality, stress, low fitness, problems at work/home or other sicknesses and medical conditions.
These factors can bring on episodes of back pain or increase symptom severity. Physiotherapists understand the complexities of lower back pain and try to address all the contributing factors in our treatment.
I also have pain in my buttock or running down my leg from my back. What does that mean?
Leg symptoms associated with lower back pain, often referred to as “sciatica”, can be due to either somatic referred pain or radicular referred pain, both of which are described below. Physiotherapists are trained to use specific tests to determine the cause of leg symptoms and treat them appropriately.
Somatic referred pain is the most common cause of leg symptoms in patients with lower back pain and is often the cause of pain in the buttock or back of the thigh. The symptoms are due to referred pain, where the pain sensations from the lower back are mixed with the sensations from the leg. In this case there is no direct compression or irritation of the nerve roots that exit the spine, it is simply due to “cross-talk” between the sensory nerves coming from the muscles/joints of the back and those coming from the muscles/skin of the legs. This phenomenon occurs in many other areas of the body, such as shoulder symptoms with neck pain or thigh/knee symptoms with hip pain. Somatic referred pain is not associated with any loss of sensation or weakness in the legs.
Radicular referred pain is the term used to describe symptoms in the leg that are due to compression or irritation of a nerve root in the lower back. The nerve root may be physically obstructed by a disc, bone or ligament in the spine, or may be irritated by the inflammatory chemicals that are associated with an injury to one of these structures. Pain in the leg will often follow a “dermatomal” pattern, where the symptoms travel in a line from the lower back down to the foot. There may also be numbness of the skin or weakness of the muscles that are supplied by affected nerve root. It is essential that radicular referral pain is assessed thoroughly by a trained professional such as a physiotherapist, as these nerve injuries can lead to weakness that can be longstanding.
Should I get a scan for my lower back pain?
For the vast majority of people a scan is unnecessary. For most cases of lower back pain, a comprehensive physiotherapy assessment provides all the information we need to treat your pain effectively.
Imaging of the lower back can sometimes be confusing. We know that many abnormalities seen on scans do not actually cause symptoms, and many people without lower back pain will have similar ‘abnormalities’. One large scientific study found that 50% of people over the age of 30 WITHOUT back pain had disc problems! And that prevalence increased with age. If we treated everyone based solely on what was evident on the scan, the real problem could be missed and hence would not improve. In cases where our examination indicates a serious pathology, we will refer you for a scan and/or to a specialist for further examination.
How can physiotherapy help my lower back pain?
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
The lower back or “lumbar spine”, consists of 5 vertebrae (bones) in the lowest part of the spine. Lower back pain is a common condition that most of us will experience at some stage in our lives.
There are several different causes of lower back pain, with the vast majority of cases being of musculoskeletal origin without any serious structural damage. These cases respond very well to physiotherapy, which will usually include manual therapy, exercises and activity/postural modifications.
Very rarely, a person’s lower back pain may be a symptom of a more serious underlying problem. In such cases, a physiotherapist is able to assess the problem and refer to the correct medical practitioner for appropriate care.
What is causing my lower back pain?
In many cases of lower back pain, it is difficult to identify exactly which structure is causing the pain. During our examination, the first step will be to rule out anything serious.
We will test the spine’s function and decide where there are restrictions in movement or muscle contraction. Back pain is usually caused by a combination of structures and movement patterns rather than one specific joint, disc or muscle. Therefore, trying to pinpoint one specific structure as the cause of the symptoms is often misleading. We base our treatment both on the presenting symptoms as well as movement and activation patterns of the back. We aim to improve function, leading to an immediate reduction in pain and restore normal pain-free movement. There are other factors that are frequently associated with lower back pain, particularly when a person has longstanding or recurrent symptoms.
These may include poor sleep quality, stress, low fitness, problems at work/home or other sicknesses and medical conditions.
These factors can bring on episodes of back pain or increase symptom severity. Physiotherapists understand the complexities of lower back pain and try to address all the contributing factors in our treatment.
I also have pain in my buttock or running down my leg from my back. What does that mean?
Leg symptoms associated with lower back pain, often referred to as “sciatica”, can be due to either somatic referred pain or radicular referred pain, both of which are described below. Physiotherapists are trained to use specific tests to determine the cause of leg symptoms and treat them appropriately.
Somatic referred pain is the most common cause of leg symptoms in patients with lower back pain and is often the cause of pain in the buttock or back of the thigh. The symptoms are due to referred pain, where the pain sensations from the lower back are mixed with the sensations from the leg. In this case there is no direct compression or irritation of the nerve roots that exit the spine, it is simply due to “cross-talk” between the sensory nerves coming from the muscles/joints of the back and those coming from the muscles/skin of the legs. This phenomenon occurs in many other areas of the body, such as shoulder symptoms with neck pain or thigh/knee symptoms with hip pain. Somatic referred pain is not associated with any loss of sensation or weakness in the legs.
Radicular referred pain is the term used to describe symptoms in the leg that are due to compression or irritation of a nerve root in the lower back. The nerve root may be physically obstructed by a disc, bone or ligament in the spine, or may be irritated by the inflammatory chemicals that are associated with an injury to one of these structures. Pain in the leg will often follow a “dermatomal” pattern, where the symptoms travel in a line from the lower back down to the foot. There may also be numbness of the skin or weakness of the muscles that are supplied by affected nerve root. It is essential that radicular referral pain is assessed thoroughly by a trained professional such as a physiotherapist, as these nerve injuries can lead to weakness that can be longstanding.
Should I get a scan for my lower back pain?
For the vast majority of people a scan is unnecessary. For most cases of lower back pain, a comprehensive physiotherapy assessment provides all the information we need to treat your pain effectively.
Imaging of the lower back can sometimes be confusing. We know that many abnormalities seen on scans do not actually cause symptoms, and many people without lower back pain will have similar ‘abnormalities’. One large scientific study found that 50% of people over the age of 30 WITHOUT back pain had disc problems! And that prevalence increased with age. If we treated everyone based solely on what was evident on the scan, the real problem could be missed and hence would not improve. In cases where our examination indicates a serious pathology, we will refer you for a scan and/or to a specialist for further examination.
How can physiotherapy help my lower back pain?
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Lower back pain is one of the leading causes of pain and disability around the world. Physiotherapy is very effective at managing the pain and dysfunction associated with problems in this area. Read on to see answers to a number of common questions and how physiotherapy can help you.
The lower back or “lumbar spine”, consists of 5 vertebrae (bones) in the lowest part of the spine. Lower back pain is a common condition that most of us will experience at some stage in our lives.
There are several different causes of lower back pain, with the vast majority of cases being of musculoskeletal origin without any serious structural damage. These cases respond very well to physiotherapy, which will usually include manual therapy, exercises and activity/postural modifications.
Very rarely, a person’s lower back pain may be a symptom of a more serious underlying problem. In such cases, a physiotherapist is able to assess the problem and refer to the correct medical practitioner for appropriate care.
What is causing my lower back pain?
In many cases of lower back pain, it is difficult to identify exactly which structure is causing the pain. During our examination, the first step will be to rule out anything serious.
We will test the spine’s function and decide where there are restrictions in movement or muscle contraction. Back pain is usually caused by a combination of structures and movement patterns rather than one specific joint, disc or muscle. Therefore, trying to pinpoint one specific structure as the cause of the symptoms is often misleading. We base our treatment both on the presenting symptoms as well as movement and activation patterns of the back. We aim to improve function, leading to an immediate reduction in pain and restore normal pain-free movement. There are other factors that are frequently associated with lower back pain, particularly when a person has longstanding or recurrent symptoms.
These may include poor sleep quality, stress, low fitness, problems at work/home or other sicknesses and medical conditions.
These factors can bring on episodes of back pain or increase symptom severity. Physiotherapists understand the complexities of lower back pain and try to address all the contributing factors in our treatment.
I also have pain in my buttock or running down my leg from my back. What does that mean?
Leg symptoms associated with lower back pain, often referred to as “sciatica”, can be due to either somatic referred pain or radicular referred pain, both of which are described below. Physiotherapists are trained to use specific tests to determine the cause of leg symptoms and treat them appropriately.
Somatic referred pain is the most common cause of leg symptoms in patients with lower back pain and is often the cause of pain in the buttock or back of the thigh. The symptoms are due to referred pain, where the pain sensations from the lower back are mixed with the sensations from the leg. In this case there is no direct compression or irritation of the nerve roots that exit the spine, it is simply due to “cross-talk” between the sensory nerves coming from the muscles/joints of the back and those coming from the muscles/skin of the legs. This phenomenon occurs in many other areas of the body, such as shoulder symptoms with neck pain or thigh/knee symptoms with hip pain. Somatic referred pain is not associated with any loss of sensation or weakness in the legs.
Radicular referred pain is the term used to describe symptoms in the leg that are due to compression or irritation of a nerve root in the lower back. The nerve root may be physically obstructed by a disc, bone or ligament in the spine, or may be irritated by the inflammatory chemicals that are associated with an injury to one of these structures. Pain in the leg will often follow a “dermatomal” pattern, where the symptoms travel in a line from the lower back down to the foot. There may also be numbness of the skin or weakness of the muscles that are supplied by affected nerve root. It is essential that radicular referral pain is assessed thoroughly by a trained professional such as a physiotherapist, as these nerve injuries can lead to weakness that can be longstanding.
Should I get a scan for my lower back pain?
For the vast majority of people a scan is unnecessary. For most cases of lower back pain, a comprehensive physiotherapy assessment provides all the information we need to treat your pain effectively.
Imaging of the lower back can sometimes be confusing. We know that many abnormalities seen on scans do not actually cause symptoms, and many people without lower back pain will have similar ‘abnormalities’. One large scientific study found that 50% of people over the age of 30 WITHOUT back pain had disc problems! And that prevalence increased with age. If we treated everyone based solely on what was evident on the scan, the real problem could be missed and hence would not improve. In cases where our examination indicates a serious pathology, we will refer you for a scan and/or to a specialist for further examination.
How can physiotherapy help my lower back pain?
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Recoommendation
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.