Sports Injuries: A Brief Review

Miami's #1 Sports Physical Therapist
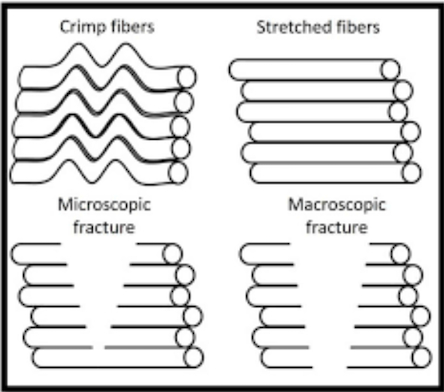
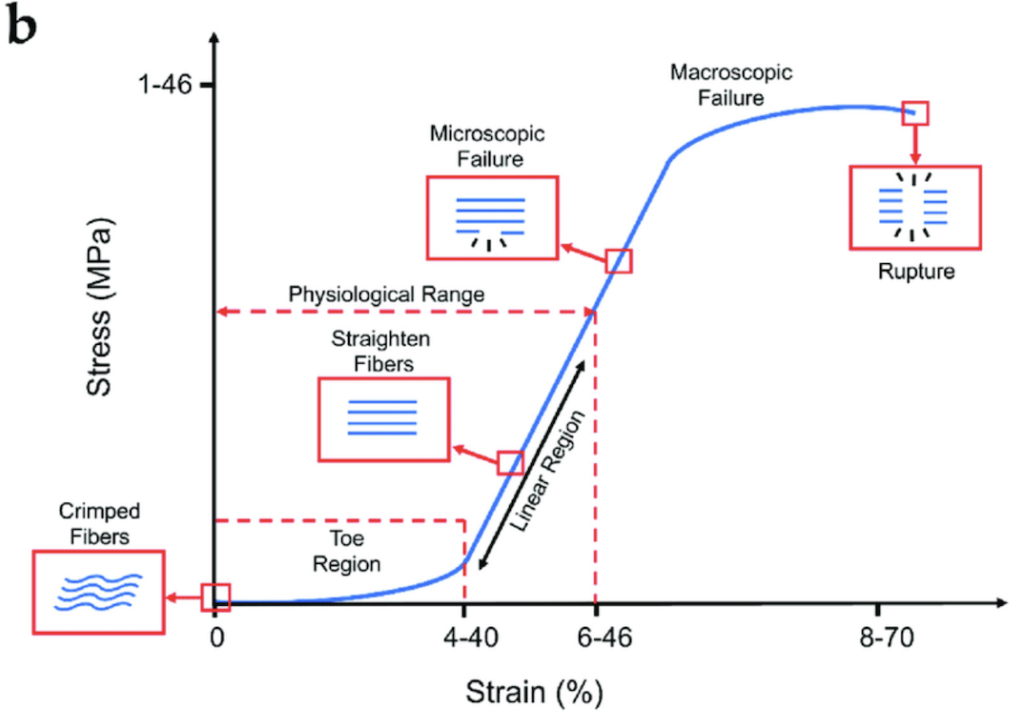
Ligaments are like rubber bands, they stretch and deform, then return to the resting position when the stimulus is removed. Ligaments have a peculiar quality in that they allow them to deform a certain amount prior to complete rupture. When injured, scar tissue may develop, altering the mechanical properties. The below picture demonstrates what happens to ligament as it is placed on stretch. First, there is an uncrimping or straightening of the fibers. If stretching continues, microscopic, then macroscopic injury may occur.
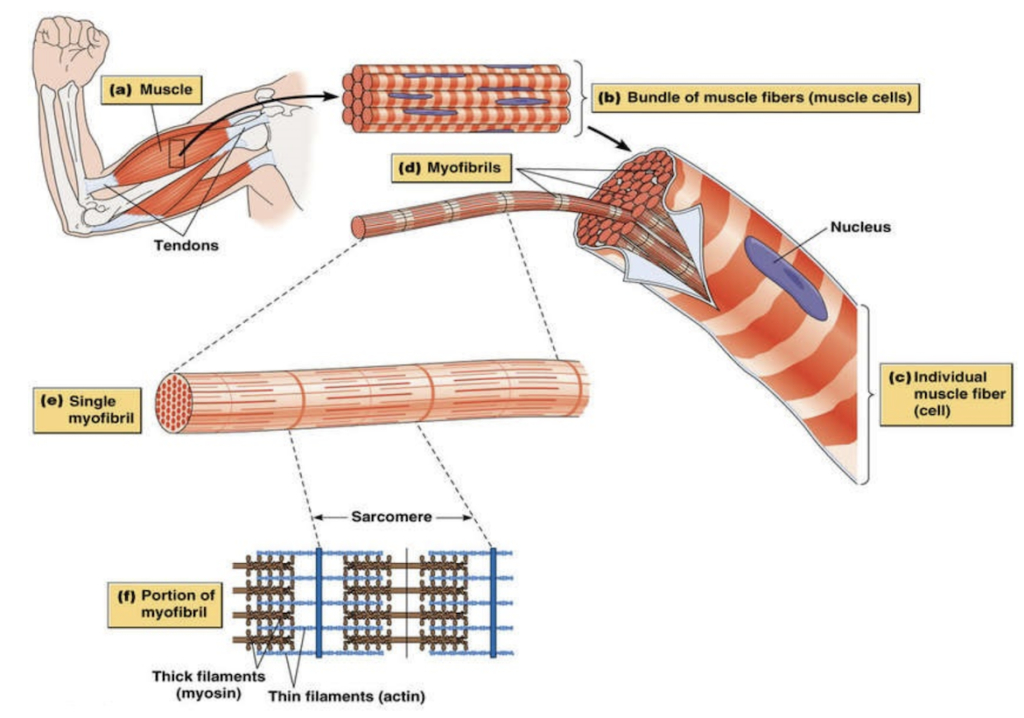
Similar to ligaments, muscle and tendons can be stretched for a certain length and time before injury occurs. With the obvious exception of muscular tissue contracts, ligaments and tendons behave in similar ways. Muscle tears can result in strength deficits and altered biomechanics. If not properly addressed, further damage may occur to the underlying bone, joints and soft tissues (cartilage, labrum, meniscus).
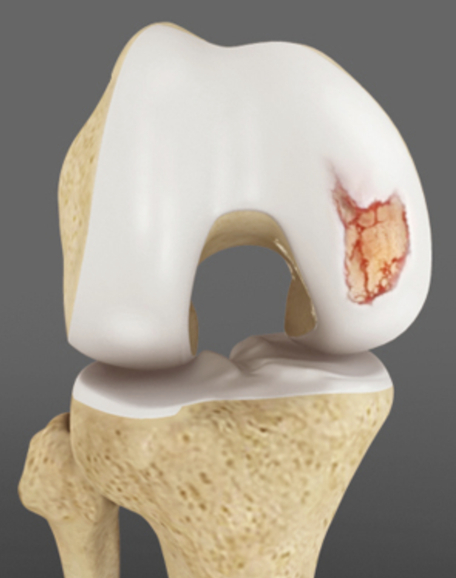
Cartilage is spongy and slippery. It acts as a shock absorber and lubricates for the joint. In the event of an injury, a piece of cartilage may fragment off the underlying bone, become a “loose body” in the joint space. If this fragment gets caught between the joint surfaces when loaded, it may cause further damage. Overtime, the joint surface undergoes degenerative changes on top of the acute trauma the loose body is causing. While degenerative joints are typical in the mid-30s and beyond, they can be treated successfully with conservative care physical therapy. Loose bodies may require surgical intervention if limitation in range of motion are observed.
The above information is a general guide for an athlete. These are the injuries that often limit participation in sports. Combat sports such as wrestling, jiu jitsu, Muay Thai or field sports like soccer, football may experience specific types of injuries or different injury rates, but the general idea is the same. Sports related injuries most often include the bones, tendons, muscles, ligaments and joints. An athlete may experience multiple injuries at once (cartilage damage in addition to a muscle strain for example). While this may complicate the recovery process, a skilled physical therapist can facilitate the rehabilitation process by having open communication with the athlete, their coaches, family and other health care providers.
The first step in return to sport is having a proper sport-specific examination by a physical therapist. After the examination, the physical therapist should explain their findings, answer any questions and then develop a plan of care specific to the needs of the athlete.
At Dr. Abbate Physical Therapy in Miami, FL, we take the time to assess and discuss your needs as an athlete to help get you back on track with your sport!
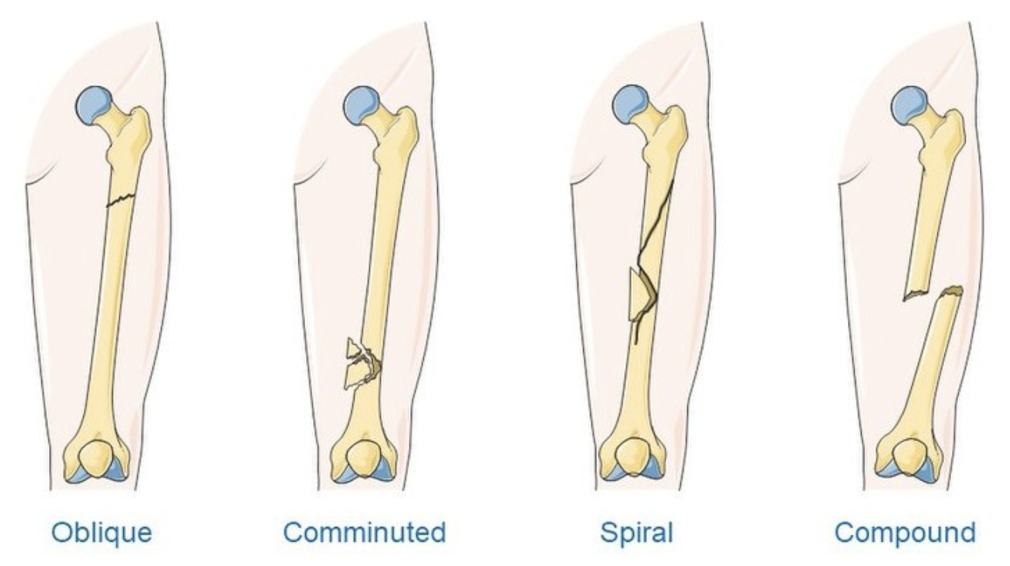
High impact or successive impacts of a time without proper healing of tissue, will result in a bone fracture. Yes, this is the same thing as a bone “breaking”. Fractures are exquisitely painful, with the individual bracing the limb from moving. Stress fractures may occur when repeated stress is introduced (like running or jumping) and proper bone remodeling does not take place. Most fractures require a period of rest. A bone stimulator is maybe used or surgery may be warranted depending on the extent of the injury.
Ligaments are like rubber bands, they stretch and deform, then return to the resting position when the stimulus is removed. Ligaments have a peculiar quality in that they allow them to deform a certain amount prior to complete rupture. When injured, scar tissue may develop, altering the mechanical properties. The below picture demonstrates what happens to ligament as it is placed on stretch. First, there is an uncrimping or straightening of the fibers. If stretching continues, microscopic, then macroscopic injury may occur.
Similar to ligaments, muscle and tendons can be stretched for a certain length and time before injury occurs. With the obvious exception of muscular tissue contracts, ligaments and tendons behave in similar ways. Muscle tears can result in strength deficits and altered biomechanics. If not properly addressed, further damage may occur to the underlying bone, joints and soft tissues (cartilage, labrum, meniscus).
Cartilage is spongy and slippery. It acts as a shock absorber and lubricates for the joint. In the event of an injury, a piece of cartilage may fragment off the underlying bone, become a “loose body” in the joint space. If this fragment gets caught between the joint surfaces when loaded, it may cause further damage. Overtime, the joint surface undergoes degenerative changes on top of the acute trauma the loose body is causing. While degenerative joints are typical in the mid-30s and beyond, they can be treated successfully with conservative care physical therapy. Loose bodies may require surgical intervention if limitation in range of motion are observed.
The above information is a general guide for an athlete. These are the injuries that often limit participation in sports. Combat sports such as wrestling, jiu jitsu, Muay Thai or field sports like soccer, football may experience specific types of injuries or different injury rates, but the general idea is the same. Sports related injuries most often include the bones, tendons, muscles, ligaments and joints. An athlete may experience multiple injuries at once (cartilage damage in addition to a muscle strain for example). While this may complicate the recovery process, a skilled physical therapist can facilitate the rehabilitation process by having open communication with the athlete, their coaches, family and other health care providers.
The first step in return to sport is having a proper sport-specific examination by a physical therapist. After the examination, the physical therapist should explain their findings, answer any questions and then develop a plan of care specific to the needs of the athlete.
At Dr. Abbate Physical Therapy in Miami, FL, we take the time to assess and discuss your needs as an athlete to help get you back on track with your sport!
With sports participation comes the inherent risk of injury. The majority of athletes will experience at least one injury in their career. Injuries are defined as some period of time off from full participation in sport. Often, many athletes will “grit through” the pain and continue to participate regardless of the work capacity of the injured body part.
Many different types of injuries can occur in sport these can be categorized as acute (bone fracture, ligament rupture), chronic (cartilage degeneration) or acute on chronic (former ligament tear reinjured and now fully ruptured, or a ligament tear that causes degeneration of the cartilage).
Acute and chronic injuries can elicit pain, resulting in loss of flexibility, muscular weakness or fear avoidance behaviors. Very often, the athlete will subconsciously alter their movements to avoid the painful position. Overtime, this may cause other problems to arise other movements will change stress patterns going through a limb. If the structure is not accustomed to the stress, injury may result.
High impact or successive impacts of a time without proper healing of tissue, will result in a bone fracture. Yes, this is the same thing as a bone “breaking”. Fractures are exquisitely painful, with the individual bracing the limb from moving. Stress fractures may occur when repeated stress is introduced (like running or jumping) and proper bone remodeling does not take place. Most fractures require a period of rest. A bone stimulator is maybe used or surgery may be warranted depending on the extent of the injury.
Ligaments are like rubber bands, they stretch and deform, then return to the resting position when the stimulus is removed. Ligaments have a peculiar quality in that they allow them to deform a certain amount prior to complete rupture. When injured, scar tissue may develop, altering the mechanical properties. The below picture demonstrates what happens to ligament as it is placed on stretch. First, there is an uncrimping or straightening of the fibers. If stretching continues, microscopic, then macroscopic injury may occur.
Similar to ligaments, muscle and tendons can be stretched for a certain length and time before injury occurs. With the obvious exception of muscular tissue contracts, ligaments and tendons behave in similar ways. Muscle tears can result in strength deficits and altered biomechanics. If not properly addressed, further damage may occur to the underlying bone, joints and soft tissues (cartilage, labrum, meniscus).
Cartilage is spongy and slippery. It acts as a shock absorber and lubricates for the joint. In the event of an injury, a piece of cartilage may fragment off the underlying bone, become a “loose body” in the joint space. If this fragment gets caught between the joint surfaces when loaded, it may cause further damage. Overtime, the joint surface undergoes degenerative changes on top of the acute trauma the loose body is causing. While degenerative joints are typical in the mid-30s and beyond, they can be treated successfully with conservative care physical therapy. Loose bodies may require surgical intervention if limitation in range of motion are observed.
The above information is a general guide for an athlete. These are the injuries that often limit participation in sports. Combat sports such as wrestling, jiu jitsu, Muay Thai or field sports like soccer, football may experience specific types of injuries or different injury rates, but the general idea is the same. Sports related injuries most often include the bones, tendons, muscles, ligaments and joints. An athlete may experience multiple injuries at once (cartilage damage in addition to a muscle strain for example). While this may complicate the recovery process, a skilled physical therapist can facilitate the rehabilitation process by having open communication with the athlete, their coaches, family and other health care providers.
The first step in return to sport is having a proper sport-specific examination by a physical therapist. After the examination, the physical therapist should explain their findings, answer any questions and then develop a plan of care specific to the needs of the athlete.
At Dr. Abbate Physical Therapy in Miami, FL, we take the time to assess and discuss your needs as an athlete to help get you back on track with your sport!
The arm bar is a joint lock of the elbow. On the posterior (back side) and lateral (outside) of the elbow, the sensitive joint surfaces are aggressively pressed together, resulting in pain. On the anterior (front) of the elbow, several ligaments and muscles are strained. Injuries involving the arm bar often result in poor range of motion (inability to fully straighten the arm) and weakness with pushing or pulling.

The wrist lock is another type of joint lock. The wrist is maximally flexed to the end range of motion, resulting in compression of the joints on the palmar side of the hand, and over-stretching of the muscles, tendons and ligaments on the dorsum of the hand (back of the hand). The injury may result in a condition called scapholunate instability, resulting in pain with wrist movement and gripping. In rare circumstances, if the blood supply to the scaphoid bone is compromised, the bone may be affected.

The knee bar is a joint lock of the knee. The muscles and ligaments of the posterior leg (hamstring, capsule) are over-stretched. This may result in muscle and tendon strains or ligamentous sprains. The knee may become unstable due to lack of ligamentous support, or may be weak due to muscular damage.
The heel hook is a technique that applies force to the opponents heel, rotating the lower limb on the upper limb. The rotation can disrupt ligaments or the meniscus. This is caused by maximally rotated (stretching) of the soft tissues (ligaments), while pinching the sensitive meniscus between the femoral condyle and tibial plateau.
The toe hold is a forefoot/ankle lock that places stress on the ligaments, muscle and soft tissues of the foot and ankle. The ligaments, capsule and muscles of the top (dorsum) of the foot are maximally stretched. This may result in ligament sprains, or muscle/tendon strains. On the opposite side of the joint (above the heel), the joint surfaces are compressed, resulting in joint-related pathology such as cartilage and perhaps the underlying bone.
The straight ankle is similar to the toe hold in the structures stressed and resulting injury. The only difference is in how the opponents limb is attacked.
This is a brief overview of the many types of submissions that can be applied in Brazilian Jiu-Jitsu, Judo, MMA and submission grappling. This is not an exhaustive list, it is only meant to give you an idea of what anatomical structures can be damaged with several submissions.
Combat sport athletes should be well-acquainted with these submissions to have a better understanding of how they work.
Acute and chronic sports injuries can significantly affect an athletes life span. Proper examination and treatment can make a big difference in training quality and quantity. If you are a combat sport athlete in South Florida or Miami and want a physical therapist that trains and works with high level athletes,

The Americana and Kimura are shoulder locks that stress soft tissue (labrum, capsule and ligaments) of the shoulder. At the end ranges of motion, the labrum may become wedged between the head of the humerus and the underlying bone of the glenoid fossa (which the labrum attaches to). At the end range of motion, the ligaments on the opposite side of the joint (that which the movement is directed away from) are maximally stretched. The result is either degeneration of the labrum or a torn ligament. These types of injuries often result in shoulder instability as both structures are responsible for maintaining the glenohumeral joint intact.
The arm bar is a joint lock of the elbow. On the posterior (back side) and lateral (outside) of the elbow, the sensitive joint surfaces are aggressively pressed together, resulting in pain. On the anterior (front) of the elbow, several ligaments and muscles are strained. Injuries involving the arm bar often result in poor range of motion (inability to fully straighten the arm) and weakness with pushing or pulling.
The wrist lock is another type of joint lock. The wrist is maximally flexed to the end range of motion, resulting in compression of the joints on the palmar side of the hand, and over-stretching of the muscles, tendons and ligaments on the dorsum of the hand (back of the hand). The injury may result in a condition called scapholunate instability, resulting in pain with wrist movement and gripping. In rare circumstances, if the blood supply to the scaphoid bone is compromised, the bone may be affected.
The knee bar is a joint lock of the knee. The muscles and ligaments of the posterior leg (hamstring, capsule) are over-stretched. This may result in muscle and tendon strains or ligamentous sprains. The knee may become unstable due to lack of ligamentous support, or may be weak due to muscular damage.
The heel hook is a technique that applies force to the opponents heel, rotating the lower limb on the upper limb. The rotation can disrupt ligaments or the meniscus. This is caused by maximally rotated (stretching) of the soft tissues (ligaments), while pinching the sensitive meniscus between the femoral condyle and tibial plateau.
The toe hold is a forefoot/ankle lock that places stress on the ligaments, muscle and soft tissues of the foot and ankle. The ligaments, capsule and muscles of the top (dorsum) of the foot are maximally stretched. This may result in ligament sprains, or muscle/tendon strains. On the opposite side of the joint (above the heel), the joint surfaces are compressed, resulting in joint-related pathology such as cartilage and perhaps the underlying bone.
The straight ankle is similar to the toe hold in the structures stressed and resulting injury. The only difference is in how the opponents limb is attacked.
This is a brief overview of the many types of submissions that can be applied in Brazilian Jiu-Jitsu, Judo, MMA and submission grappling. This is not an exhaustive list, it is only meant to give you an idea of what anatomical structures can be damaged with several submissions.
Combat sport athletes should be well-acquainted with these submissions to have a better understanding of how they work.
Acute and chronic sports injuries can significantly affect an athletes life span. Proper examination and treatment can make a big difference in training quality and quantity. If you are a combat sport athlete in South Florida or Miami and want a physical therapist that trains and works with high level athletes,
Chokes to the neck are brought on by occlusion (closing off) of blood vessels that supply the brain with blood. The result is a loss of consciousness if the person does not tap. This is a very effective form of submission, since it establishes a clear advantage. Once the choke is relieved, no significant lasting damage occurs. However, in the case that the choke is continued, irreversible damage to the brain, or death, may occur.
The Americana and Kimura are shoulder locks that stress soft tissue (labrum, capsule and ligaments) of the shoulder. At the end ranges of motion, the labrum may become wedged between the head of the humerus and the underlying bone of the glenoid fossa (which the labrum attaches to). At the end range of motion, the ligaments on the opposite side of the joint (that which the movement is directed away from) are maximally stretched. The result is either degeneration of the labrum or a torn ligament. These types of injuries often result in shoulder instability as both structures are responsible for maintaining the glenohumeral joint intact.
The arm bar is a joint lock of the elbow. On the posterior (back side) and lateral (outside) of the elbow, the sensitive joint surfaces are aggressively pressed together, resulting in pain. On the anterior (front) of the elbow, several ligaments and muscles are strained. Injuries involving the arm bar often result in poor range of motion (inability to fully straighten the arm) and weakness with pushing or pulling.
The wrist lock is another type of joint lock. The wrist is maximally flexed to the end range of motion, resulting in compression of the joints on the palmar side of the hand, and over-stretching of the muscles, tendons and ligaments on the dorsum of the hand (back of the hand). The injury may result in a condition called scapholunate instability, resulting in pain with wrist movement and gripping. In rare circumstances, if the blood supply to the scaphoid bone is compromised, the bone may be affected.
The knee bar is a joint lock of the knee. The muscles and ligaments of the posterior leg (hamstring, capsule) are over-stretched. This may result in muscle and tendon strains or ligamentous sprains. The knee may become unstable due to lack of ligamentous support, or may be weak due to muscular damage.
The heel hook is a technique that applies force to the opponents heel, rotating the lower limb on the upper limb. The rotation can disrupt ligaments or the meniscus. This is caused by maximally rotated (stretching) of the soft tissues (ligaments), while pinching the sensitive meniscus between the femoral condyle and tibial plateau.
The toe hold is a forefoot/ankle lock that places stress on the ligaments, muscle and soft tissues of the foot and ankle. The ligaments, capsule and muscles of the top (dorsum) of the foot are maximally stretched. This may result in ligament sprains, or muscle/tendon strains. On the opposite side of the joint (above the heel), the joint surfaces are compressed, resulting in joint-related pathology such as cartilage and perhaps the underlying bone.
The straight ankle is similar to the toe hold in the structures stressed and resulting injury. The only difference is in how the opponents limb is attacked.
This is a brief overview of the many types of submissions that can be applied in Brazilian Jiu-Jitsu, Judo, MMA and submission grappling. This is not an exhaustive list, it is only meant to give you an idea of what anatomical structures can be damaged with several submissions.
Combat sport athletes should be well-acquainted with these submissions to have a better understanding of how they work.
Acute and chronic sports injuries can significantly affect an athletes life span. Proper examination and treatment can make a big difference in training quality and quantity. If you are a combat sport athlete in South Florida or Miami and want a physical therapist that trains and works with high level athletes,
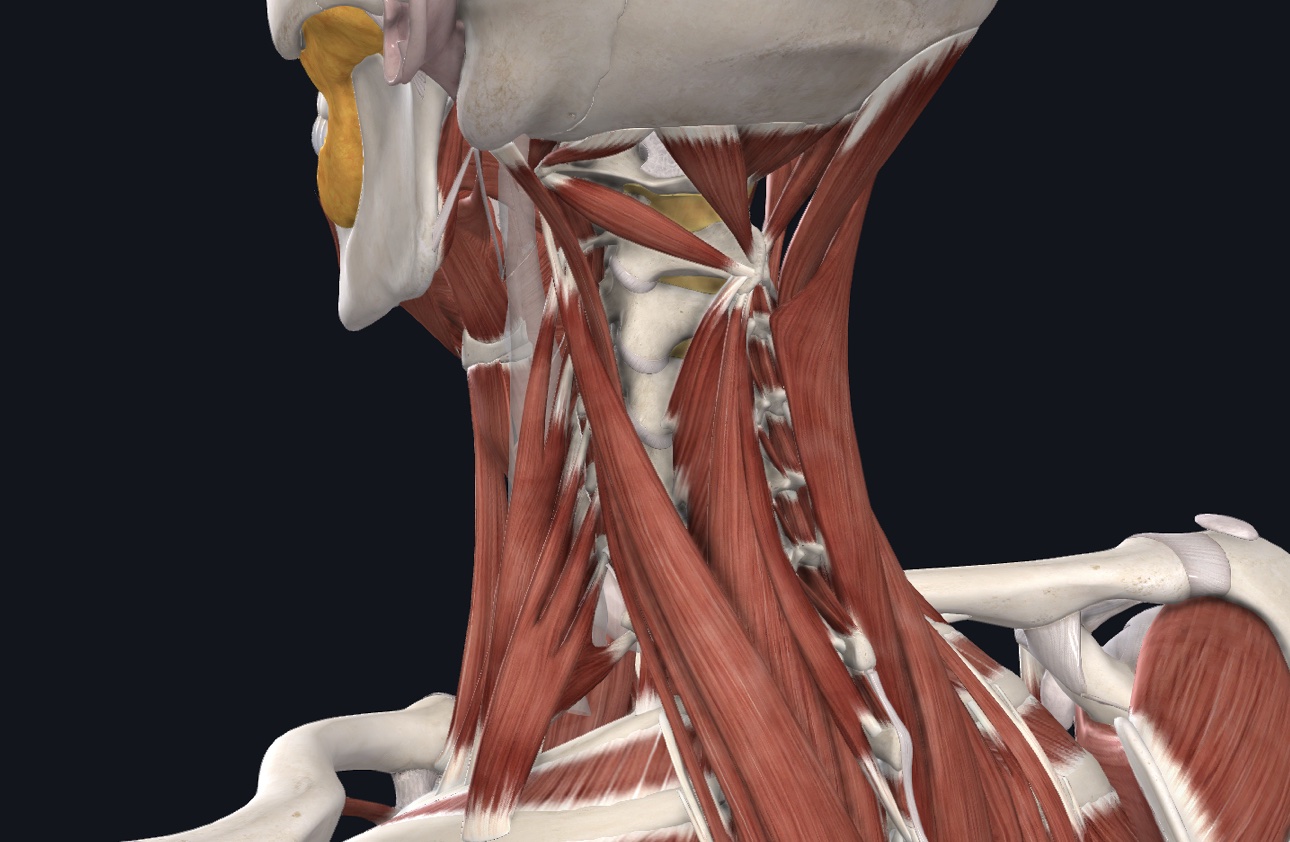
The neck crank is when direct pressure is applied to the opponents neck via a choke hold. The pressure on the sensitive bone and other soft tissues (muscles, joint surfaces) reproduces exquisite pain. Since the neck has the important task of maintaining head position when moving, gaze stabilization and proprioception among other things, the “wiring” is quite sensitive to pain.
Chokes to the neck are brought on by occlusion (closing off) of blood vessels that supply the brain with blood. The result is a loss of consciousness if the person does not tap. This is a very effective form of submission, since it establishes a clear advantage. Once the choke is relieved, no significant lasting damage occurs. However, in the case that the choke is continued, irreversible damage to the brain, or death, may occur.
The Americana and Kimura are shoulder locks that stress soft tissue (labrum, capsule and ligaments) of the shoulder. At the end ranges of motion, the labrum may become wedged between the head of the humerus and the underlying bone of the glenoid fossa (which the labrum attaches to). At the end range of motion, the ligaments on the opposite side of the joint (that which the movement is directed away from) are maximally stretched. The result is either degeneration of the labrum or a torn ligament. These types of injuries often result in shoulder instability as both structures are responsible for maintaining the glenohumeral joint intact.
The arm bar is a joint lock of the elbow. On the posterior (back side) and lateral (outside) of the elbow, the sensitive joint surfaces are aggressively pressed together, resulting in pain. On the anterior (front) of the elbow, several ligaments and muscles are strained. Injuries involving the arm bar often result in poor range of motion (inability to fully straighten the arm) and weakness with pushing or pulling.
The wrist lock is another type of joint lock. The wrist is maximally flexed to the end range of motion, resulting in compression of the joints on the palmar side of the hand, and over-stretching of the muscles, tendons and ligaments on the dorsum of the hand (back of the hand). The injury may result in a condition called scapholunate instability, resulting in pain with wrist movement and gripping. In rare circumstances, if the blood supply to the scaphoid bone is compromised, the bone may be affected.
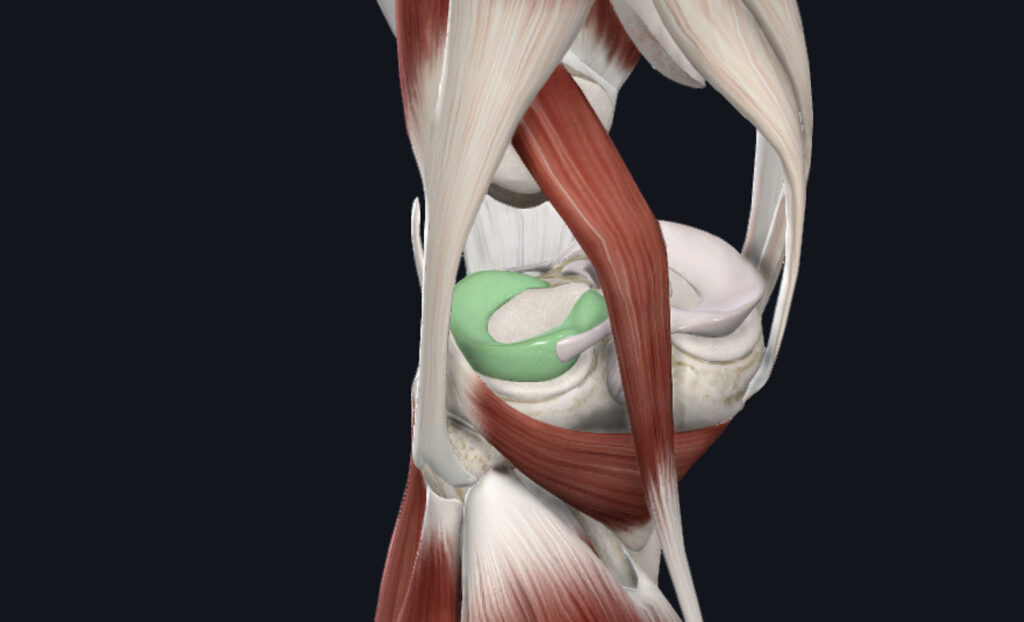
The knee bar is a joint lock of the knee. The muscles and ligaments of the posterior leg (hamstring, capsule) are over-stretched. This may result in muscle and tendon strains or ligamentous sprains. The knee may become unstable due to lack of ligamentous support, or may be weak due to muscular damage.
The heel hook is a technique that applies force to the opponents heel, rotating the lower limb on the upper limb. The rotation can disrupt ligaments or the meniscus. This is caused by maximally rotated (stretching) of the soft tissues (ligaments), while pinching the sensitive meniscus between the femoral condyle and tibial plateau.
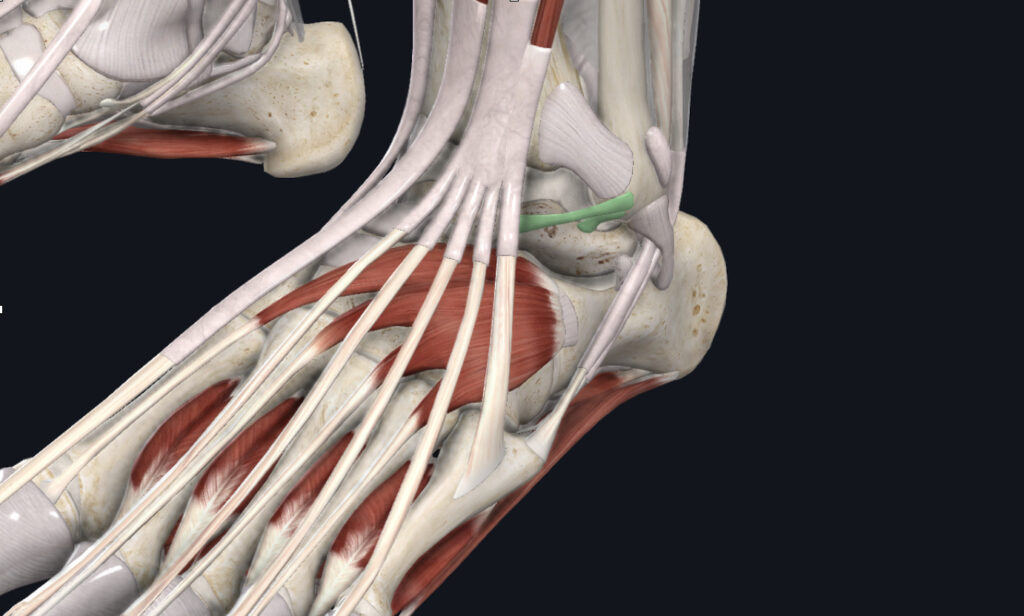
The toe hold is a forefoot/ankle lock that places stress on the ligaments, muscle and soft tissues of the foot and ankle. The ligaments, capsule and muscles of the top (dorsum) of the foot are maximally stretched. This may result in ligament sprains, or muscle/tendon strains. On the opposite side of the joint (above the heel), the joint surfaces are compressed, resulting in joint-related pathology such as cartilage and perhaps the underlying bone.
The straight ankle is similar to the toe hold in the structures stressed and resulting injury. The only difference is in how the opponents limb is attacked.
This is a brief overview of the many types of submissions that can be applied in Brazilian Jiu-Jitsu, Judo, MMA and submission grappling. This is not an exhaustive list, it is only meant to give you an idea of what anatomical structures can be damaged with several submissions.
Combat sport athletes should be well-acquainted with these submissions to have a better understanding of how they work.
Acute and chronic sports injuries can significantly affect an athletes life span. Proper examination and treatment can make a big difference in training quality and quantity. If you are a combat sport athlete in South Florida or Miami and want a physical therapist that trains and works with high level athletes,
Are you a combat sport athlete and want to learn more about what structures are affected when applying chokes, cranks and joint locks?
Here is a brief overview.
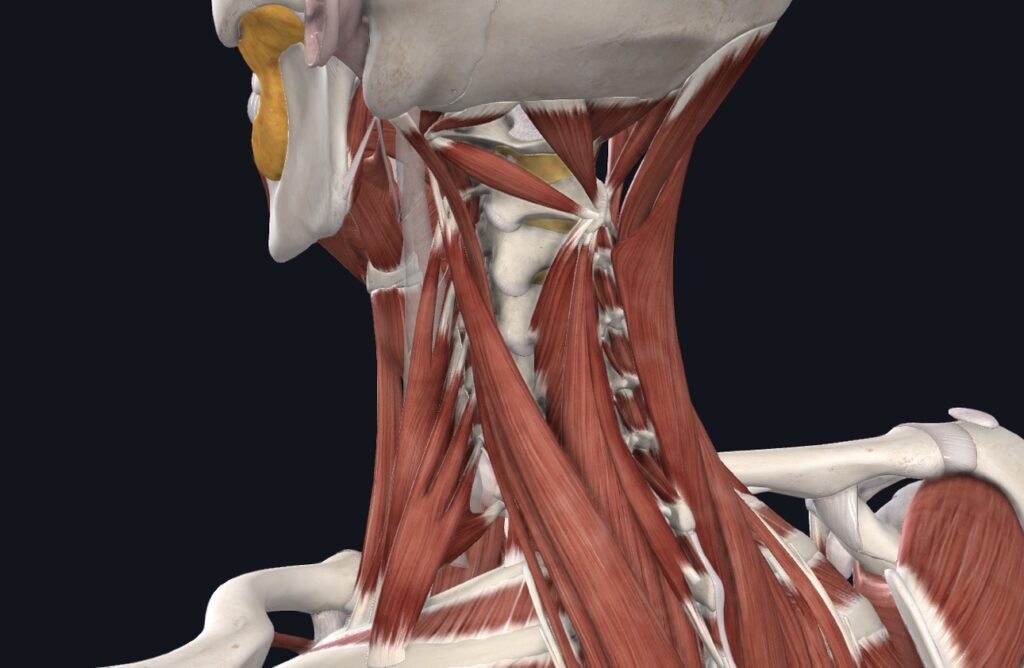
The neck crank is when direct pressure is applied to the opponents neck via a choke hold. The pressure on the sensitive bone and other soft tissues (muscles, joint surfaces) reproduces exquisite pain. Since the neck has the important task of maintaining head position when moving, gaze stabilization and proprioception among other things, the “wiring” is quite sensitive to pain.
Chokes to the neck are brought on by occlusion (closing off) of blood vessels that supply the brain with blood. The result is a loss of consciousness if the person does not tap. This is a very effective form of submission, since it establishes a clear advantage. Once the choke is relieved, no significant lasting damage occurs. However, in the case that the choke is continued, irreversible damage to the brain, or death, may occur.
The Americana and Kimura are shoulder locks that stress soft tissue (labrum, capsule and ligaments) of the shoulder. At the end ranges of motion, the labrum may become wedged between the head of the humerus and the underlying bone of the glenoid fossa (which the labrum attaches to). At the end range of motion, the ligaments on the opposite side of the joint (that which the movement is directed away from) are maximally stretched. The result is either degeneration of the labrum or a torn ligament. These types of injuries often result in shoulder instability as both structures are responsible for maintaining the glenohumeral joint intact.
The arm bar is a joint lock of the elbow. On the posterior (back side) and lateral (outside) of the elbow, the sensitive joint surfaces are aggressively pressed together, resulting in pain. On the anterior (front) of the elbow, several ligaments and muscles are strained. Injuries involving the arm bar often result in poor range of motion (inability to fully straighten the arm) and weakness with pushing or pulling.
The wrist lock is another type of joint lock. The wrist is maximally flexed to the end range of motion, resulting in compression of the joints on the palmar side of the hand, and over-stretching of the muscles, tendons and ligaments on the dorsum of the hand (back of the hand). The injury may result in a condition called scapholunate instability, resulting in pain with wrist movement and gripping. In rare circumstances, if the blood supply to the scaphoid bone is compromised, the bone may be affected.
The knee bar is a joint lock of the knee. The muscles and ligaments of the posterior leg (hamstring, capsule) are over-stretched. This may result in muscle and tendon strains or ligamentous sprains. The knee may become unstable due to lack of ligamentous support, or may be weak due to muscular damage.
The heel hook is a technique that applies force to the opponents heel, rotating the lower limb on the upper limb. The rotation can disrupt ligaments or the meniscus. This is caused by maximally rotated (stretching) of the soft tissues (ligaments), while pinching the sensitive meniscus between the femoral condyle and tibial plateau.
The toe hold is a forefoot/ankle lock that places stress on the ligaments, muscle and soft tissues of the foot and ankle. The ligaments, capsule and muscles of the top (dorsum) of the foot are maximally stretched. This may result in ligament sprains, or muscle/tendon strains. On the opposite side of the joint (above the heel), the joint surfaces are compressed, resulting in joint-related pathology such as cartilage and perhaps the underlying bone.
The straight ankle is similar to the toe hold in the structures stressed and resulting injury. The only difference is in how the opponents limb is attacked.
This is a brief overview of the many types of submissions that can be applied in Brazilian Jiu-Jitsu, Judo, MMA and submission grappling. This is not an exhaustive list, it is only meant to give you an idea of what anatomical structures can be damaged with several submissions.
Combat sport athletes should be well-acquainted with these submissions to have a better understanding of how they work.
Acute and chronic sports injuries can significantly affect an athletes life span. Proper examination and treatment can make a big difference in training quality and quantity. If you are a combat sport athlete in South Florida or Miami and want a physical therapist that trains and works with high level athletes,
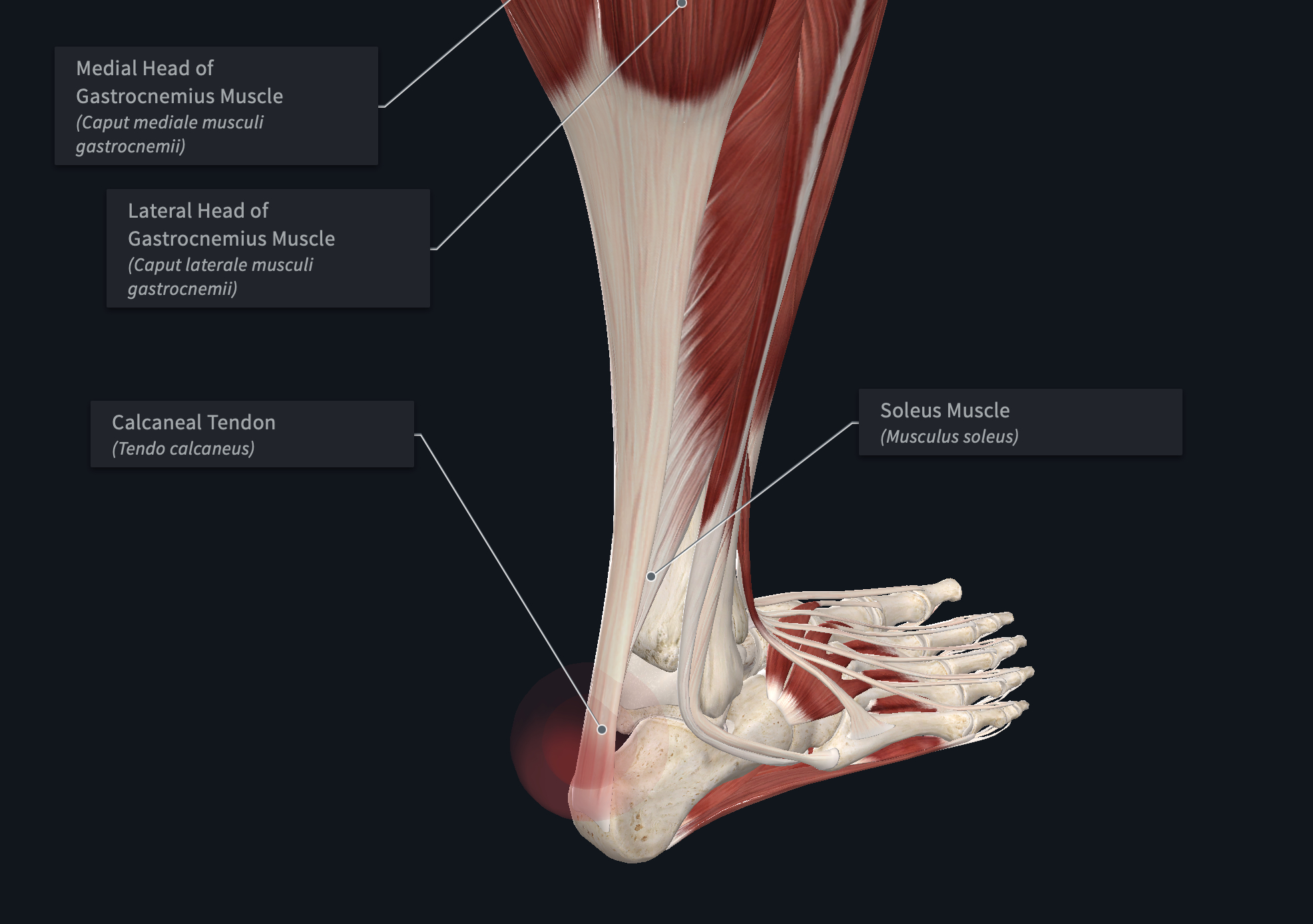
This video will describe basic anatomy of achilles tendinopathy.
Achilles tendinopathy is often described by patients as sharp (acute) or dull/aching (chronic). The pain is often made worse with rising onto the toes, jumping and running. In the early stages, there may be a “warming up” phenomenon where the pain resolved with movement. In later stages, the pain may persist for longer, requiring rest or cessation of activity.
Treatment for achilles tendinopathy often includes activity modification, mobility and strength training exercises. Some exercises are designed to manage pain when symptomatic, typically before or during exercise or sports training.
While previous medical intervention included NSAIDs for pain and sometimes corticosteroids, current models are reversing that recommendation. NSAIDs and corticosteroids, while effective at pain management, interrupt the healing process, either prolonging tissue remodeling or causing degeneration of the tendon itself.
The current best practice guidelines include activity modification, pain management exercises and progressive strength training exercises for successful return to sport.
If you are an athlete in Miami experiencing achilles tendinopathy pain and want to return to sport, give our office a call so we can help you develop a plan.

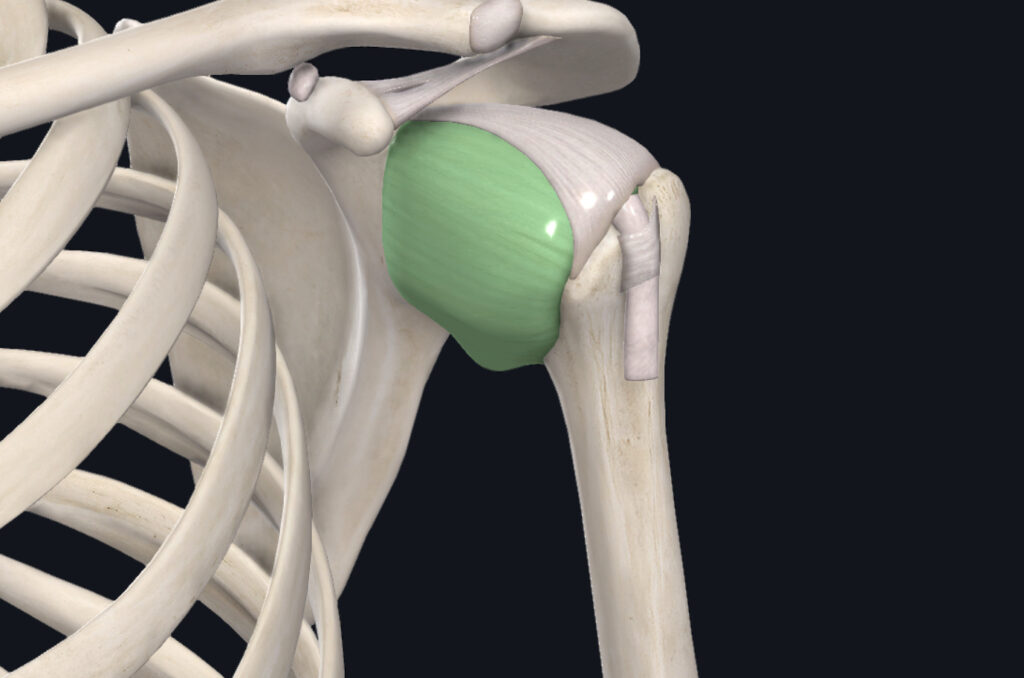
The passive structures include the joint capsule, labrum and ligaments. The joint capsule functions to provide loose structural support circumferentially as well as producing synovial fluid. The labrum provides an “lip” around the rim of the glenoid (socket) portion of the joint, stabilizing the head of the humerus (ball). The ligaments, stretching like rubber bands, provide a thickened layer in very specific areas to reinforce stability in the front, back, top and bottom. Collectively, these structures (capsule, labrum and ligaments) provide passive stability to the shoulder joint.
The active structures that provide shoulder stability include the four rotator cuff muscles (infraspinatus, subscapularis, teres minor and supraspinatus). They act to create tension as close to the joint as possible, maintaining contact between the ball and socket.
Together, these two systems act to create a stable shoulder joint throughout the available range of motion. When either of these two systems are compromised, the ball will begin to migrate excessively within the joint, possibly causing damage.
When the passive structures are compromised, as in the case of a torn labrum, or torn/chronically overstretched ligaments, the ball may ride up on the lip of the socket and damage the labrum. When this occurs, the soft surface of the ball comes into contact with the hard lip of the rim, damaging the cartilage and underlying bone.
When the active system is compromised, as in the case of a torn or weak rotator cuff muscle, a similar mechanism of injury may occur as when the passive structures are not performing properly.
The underlying cause (passive or active), extent of injury and additional pathology will determine the best course of treatment. If the injury is relatively simple (the athlete has a long history of being very mobile because they stretch a lot), then strength training usually resolves the issue. If the injury is more complex, perhaps involving a labrum tear with muscle tear, surgical intervention may be warranted. A formal evaluation by a health care provider will help determine what will best suit your particular injury.
Shoulder instability may be caused by excessive capsular laxity. The shoulder joint has two systems that create stability: actively and passively.
The passive structures include the joint capsule, labrum and ligaments. The joint capsule functions to provide loose structural support circumferentially as well as producing synovial fluid. The labrum provides an “lip” around the rim of the glenoid (socket) portion of the joint, stabilizing the head of the humerus (ball). The ligaments, stretching like rubber bands, provide a thickened layer in very specific areas to reinforce stability in the front, back, top and bottom. Collectively, these structures (capsule, labrum and ligaments) provide passive stability to the shoulder joint.
The active structures that provide shoulder stability include the four rotator cuff muscles (infraspinatus, subscapularis, teres minor and supraspinatus). They act to create tension as close to the joint as possible, maintaining contact between the ball and socket.
Together, these two systems act to create a stable shoulder joint throughout the available range of motion. When either of these two systems are compromised, the ball will begin to migrate excessively within the joint, possibly causing damage.
When the passive structures are compromised, as in the case of a torn labrum, or torn/chronically overstretched ligaments, the ball may ride up on the lip of the socket and damage the labrum. When this occurs, the soft surface of the ball comes into contact with the hard lip of the rim, damaging the cartilage and underlying bone.
When the active system is compromised, as in the case of a torn or weak rotator cuff muscle, a similar mechanism of injury may occur as when the passive structures are not performing properly.
The underlying cause (passive or active), extent of injury and additional pathology will determine the best course of treatment. If the injury is relatively simple (the athlete has a long history of being very mobile because they stretch a lot), then strength training usually resolves the issue. If the injury is more complex, perhaps involving a labrum tear with muscle tear, surgical intervention may be warranted. A formal evaluation by a health care provider will help determine what will best suit your particular injury.
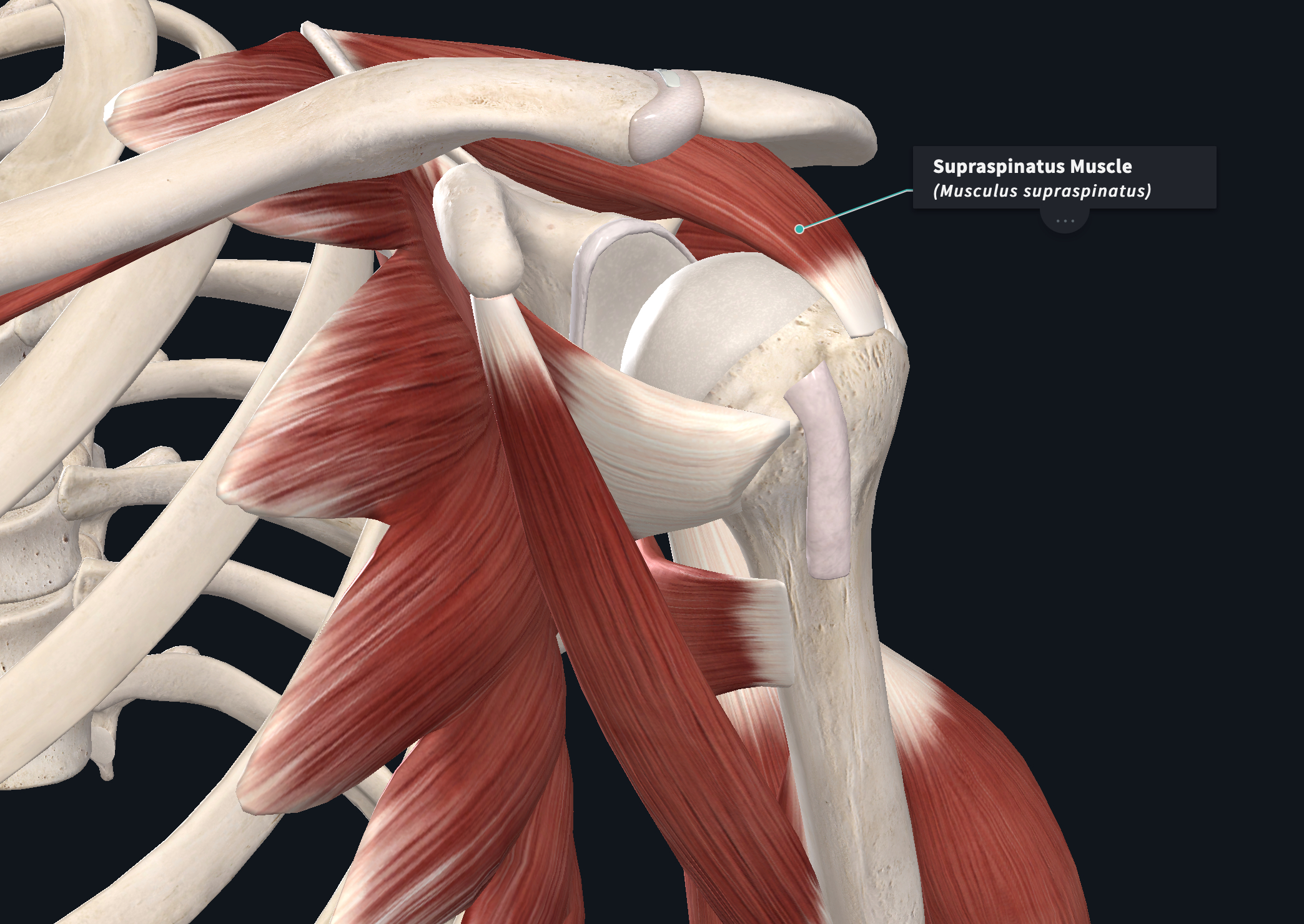
This video describes the relevant anatomy of shoulder impingement.
Shoulder impingement occurs when the supraspinatus muscle (one of the rotator cuff muscles) impinges underneath the shelf of the acromion process. The symptoms are often described as sharp when reaching overhead (elevation), across the chest (horizontal adduction) or tight when reaching behind the back (functional internal rotation).
The supraspinatus may become impinged for several reasons. The pinching often results due to an alteration in biomechanics of the shoulder. Muscle weakness or changes in the passive stability of the shoulder may cause or otherwise progress the underlying condition.
Treatment for shoulder impingement focuses on resolving the underlying cause. A proper examination and plan of care developed for your specific findings is often the best approach.
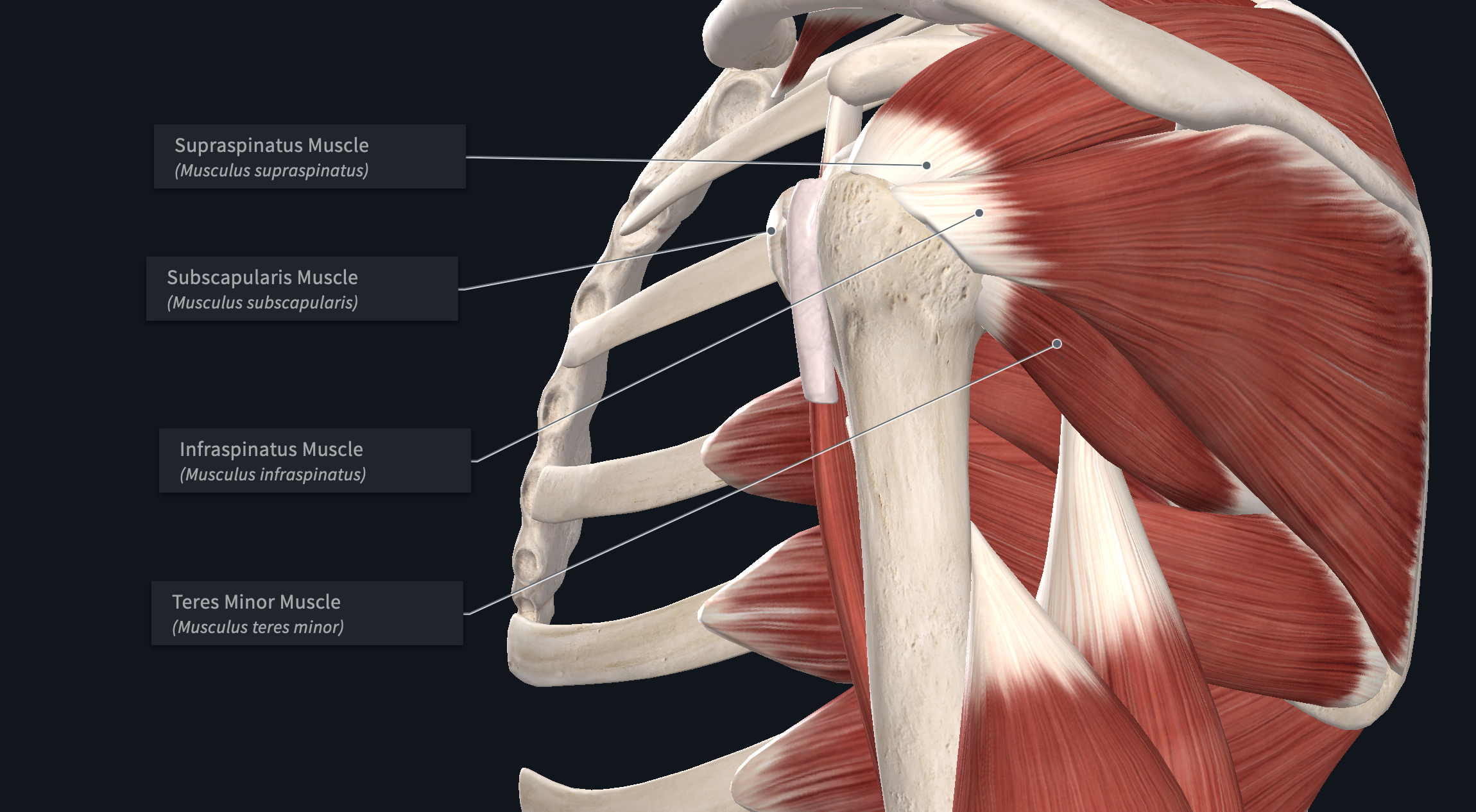
This video describes the relevant anatomy of a rotator cuff injury.
The rotator cuff is comprised of 4 muscles. As a group, these muscles act to stabilize the shoulder joint. They are generally demonstrate at least some low level of activity to provide stability to the shoulder. Depending on the position of the arm, they may contribute more or less to this stability.
One or several of the rotator cuff muscles may be injured if you fall and brace yourself with your hand (acute injury) or may become degenerated due to overtraining (chronic). Given the specificity of the rotator cuff muscles, small changes in muscle function may have profound impact on total work capacity.
Athletes often report a “pulling” sensation when the injured muscle is put to work or stretched. Other symptoms may include instability or weakness of the shoulder. Treatment for rotator cuff injuries are best determined once a physical examination is performed.
If you are an athlete in Miami, FL and experiencing shoulder pain, call our office to schedule an appointment.
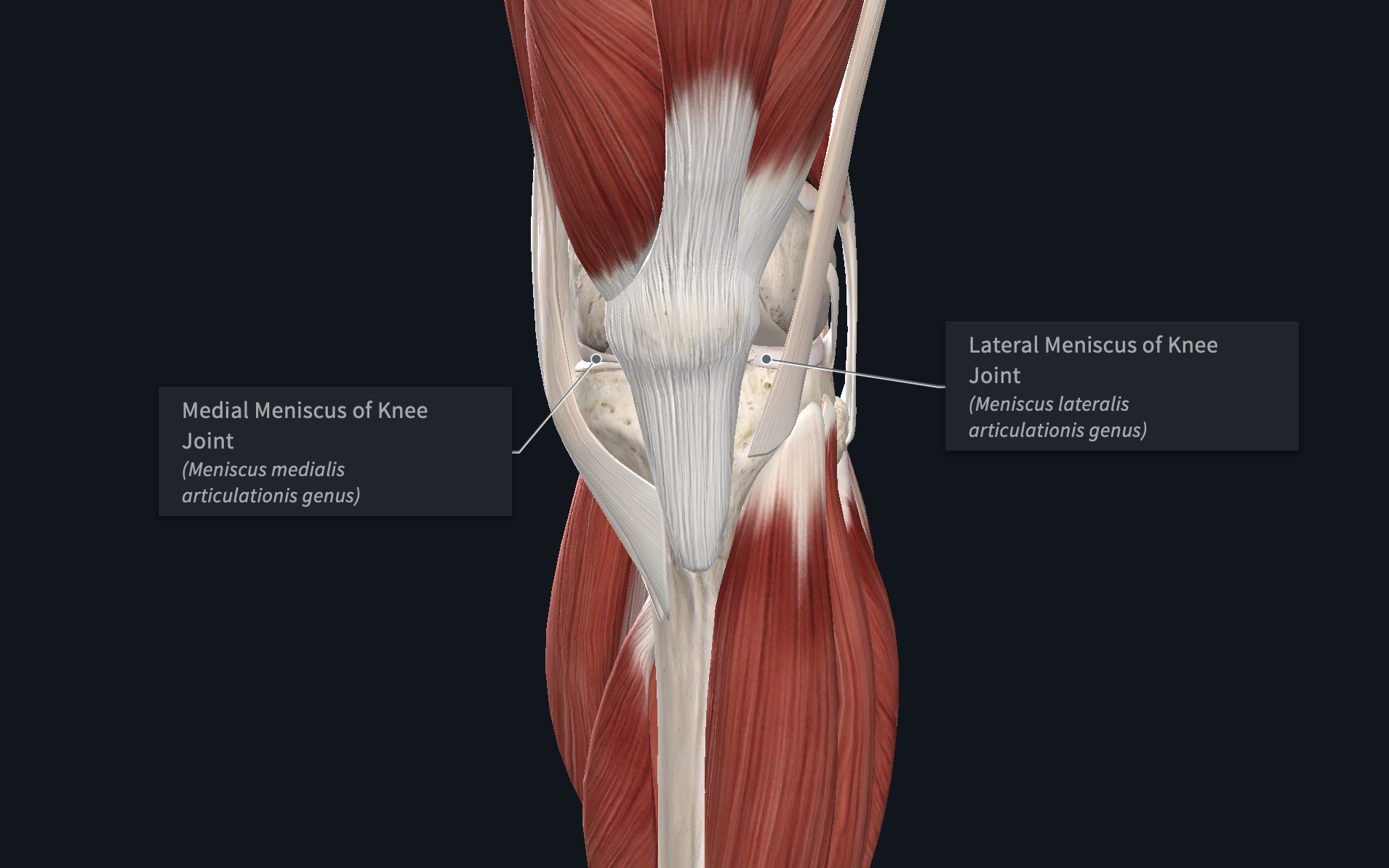
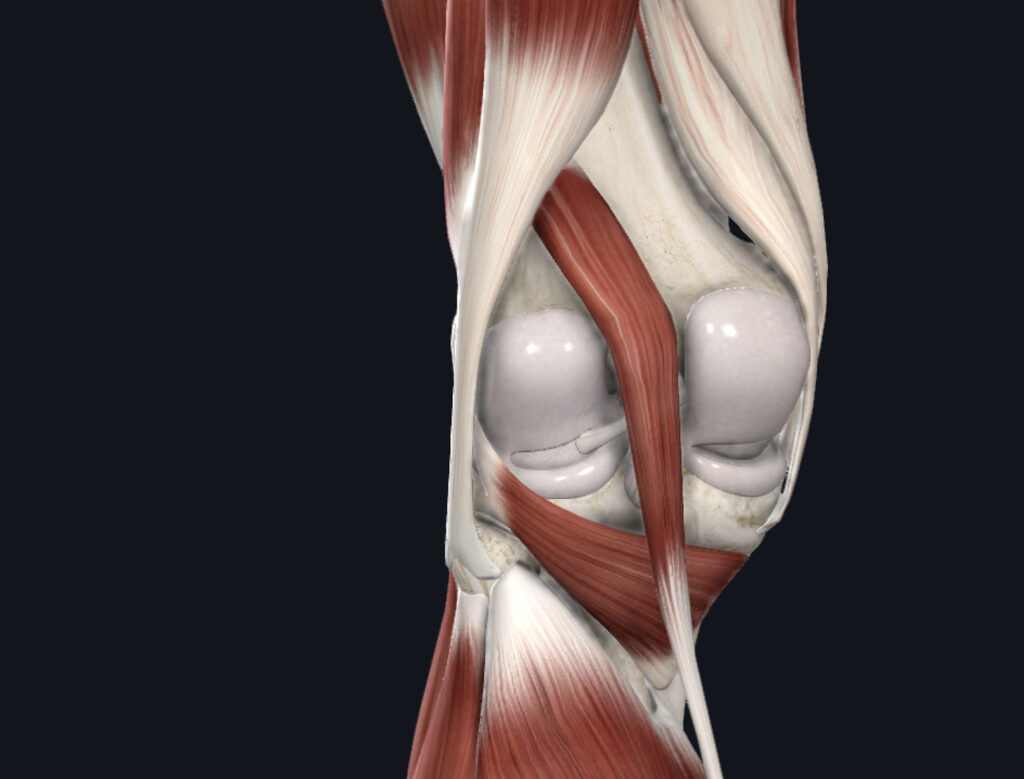
This video describes the anatomy of a meniscus injury.
The meniscus is a piece of fibrocartilage situated between the femur and tibia joint. It serves to provide a guide for movement, cushion the joint and send feedback to the brain about the position of the limb.
The meniscus is often injured when the foot is planted and the upper leg is rotated (as in pivoting). This causes compression and shearing force at the knee joint. The ligaments provide the mechanical restraints to limit excessive movement, but if they fail, the meniscus can become damaged.
Depending on the type, location and severity of the meniscus tear, symptom presentation may vary. Athletes may complain of pinching, clicking (painful or painless) of the joint or restrictions in movement (if the meniscus become caught between the joint). Treatment for meniscus tears can include conservative care (improving joint function) or surgery. The intervention you need to return to sport is best determined after a physical examination is completed by a health care provider.
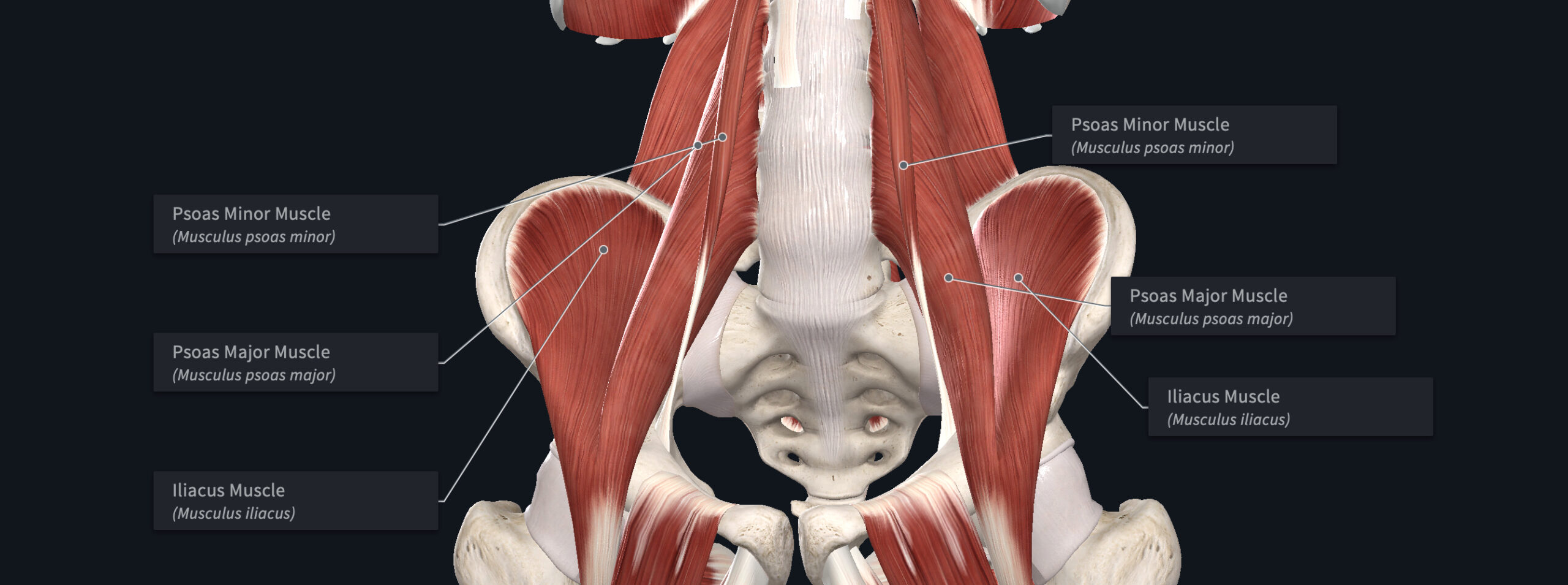
This video describes the anatomy relevant to a hip flexor strain.
The hip flexor is comprised of 2 muscles (different attachments) that form one common tendon and insert onto the femur (thigh bone). The psoas attaches onto the bones of the lumbar spine (lower back) and the iliacus attaches onto the inside surface of the pelvis. They then form one common tendon, attaching onto the upper, inner portion of the femur.
Injury to the iliopsoas (hip flexor) muscle is can result in pain with resisted hip flexion (bringing the knee to the chest), extension and activities like running and jumping. The pain may be described as sharp, snapping or dull/aching, usually in the crease of the hip. Injury of the hip flexor may be traumatic (too much resistance when performing a hip flexion activity) or chronic (overtraining).
The pain is usually localized to the front of the hip and may also present as low back pain (due to its attachment along the lumbar spine).
Treatment for a hip flexor strain usually includes activity modification (cessation of pain provoking tasks), in addition to strength and mobility training.
If you are an athlete in Miami, FL experiencing hip pain with sports activities, reach out to contact us today to schedule an appointment. A physical therapy examination can help determine and treat the root cause of pain.
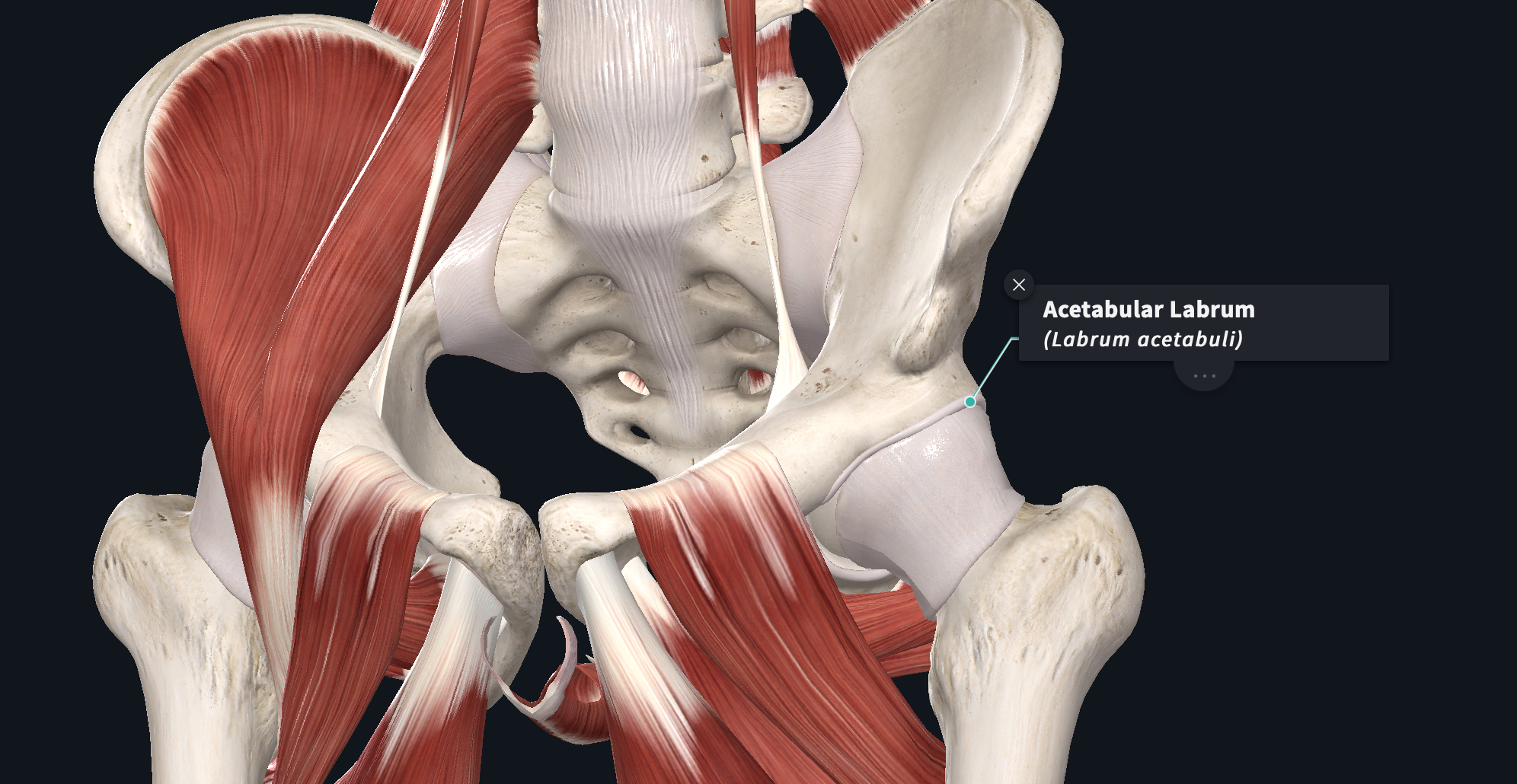
The labrum is soft and spongy. It may become “impinged” between the femur and the acetabular rim (attachment site of the labrum). Athletes often describe hip impingement as “pinching” when bringing the knee up and across the chest (hip flexion, adduction and internal rotation).
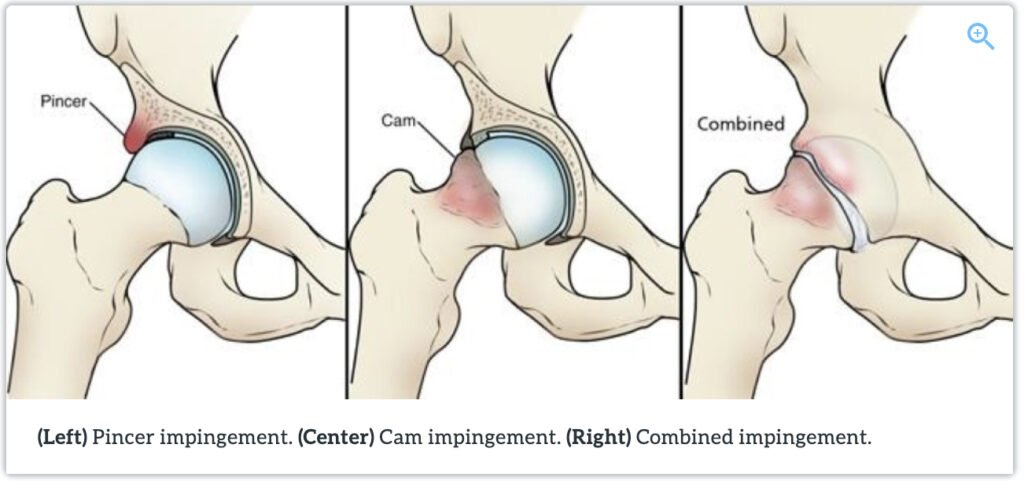
There are several causes. Acute trauma can tear the labrum, resulting in inflammation and catching inside the joint space. Chronically, a degenerative labrum can expose the underlying bone which can become bruised or otherwise degenerative as well. Some athletes have bony architecture that predispose them to this condition. Differences in femoral neck angulation, size of the femoral head compared to the acetabular fossa (socket portion of joint), and biomechanics can play a role in the development of femoroacetabular impingement.
Treatment for hip impingement should be based upon your examination. Depending on the cause, conservative care (physical therapy) or surgical intervention may be warranted.
If you are an athlete in Miami, FL experiencing hip pain with sports activities, reach out to contact us today to schedule an appointment. A physical therapy examination can help determine and treat the root cause of pain.
This video describes the relevant anatomy for femoroacetabular, or hip impingement.
Hip impingement (Femoroacetabular impingement) is caused by the compression of the labrum, a soft tissue of the hip joint. The labrum forms a “lip” around the socket part of the hip joint, providing stability, congruency and information to the brain about the joints position in space.
The labrum is soft and spongy. It may become “impinged” between the femur and the acetabular rim (attachment site of the labrum). Athletes often describe hip impingement as “pinching” when bringing the knee up and across the chest (hip flexion, adduction and internal rotation).
There are several causes. Acute trauma can tear the labrum, resulting in inflammation and catching inside the joint space. Chronically, a degenerative labrum can expose the underlying bone which can become bruised or otherwise degenerative as well. Some athletes have bony architecture that predispose them to this condition. Differences in femoral neck angulation, size of the femoral head compared to the acetabular fossa (socket portion of joint), and biomechanics can play a role in the development of femoroacetabular impingement.
Treatment for hip impingement should be based upon your examination. Depending on the cause, conservative care (physical therapy) or surgical intervention may be warranted.
If you are an athlete in Miami, FL experiencing hip pain with sports activities, reach out to contact us today to schedule an appointment. A physical therapy examination can help determine and treat the root cause of pain.

Youth athletes participating in sport offer many benefits including development of self-esteem, peer socialization and general fitness. The opportunity for scholarships and a future career places an emphasis on early competitive success. Research demonstrates that early intensity training and competition can lead to overuse injury and burnout.
Health care professionals, and sports physical therapists in particular, are trained to recognize young athletes at risk for overuse injury and burnout. Overuse injuries occur due to repetitive loading of tissue without adequate rest (too much training, not enough rest). Injuries of the muscle, tendon, bone, bursa, neurovascular structures and the physis are vulnerable. Young athletes are at particular risk for skeletal injury due to the presence of growth plates.
There are an estimated 27 million US youth athletes participating in team sports and 60 million participating in some form of organized athletics. There are 44 million youth athletes that engage in more than 1 sport. Between 45-54% of youth athletes will experience an overuse injury. However, the injury rates vary with each specific sport.
Prior injury history is a strong predictor of future overuse injury. The youth athlete is more likely to experience an injury while going through a growth spurt. The physes, apophyses and joint surfaces are less resistant to the demands of exercise compared to mature skeletons. Other factors that may contribute are a relative lack of muscle mass, joint hyper mobility and imbalance in growth and strength. In females, a history of amenorrhea is a significant risk factor for stress factors. Higher training volumes have consistently been shown to increase the risk of overuse injury in multiple sports. Poor-fitting equipment, over-scheduling and reduced recovery time also increase risk of overuse injury.
Readiness for sport should be based on individual growth and maturity. Youth athletes mature at different rates amongst their peers. Strength, balance, cognitive and social/emotional development mature within the youth athlete. Coaches and parents may lack knowledge about normal development and signs of readiness for certain tasks, physically and psychosocially. Children may lose self-esteem if coaches or parents have unrealistic expectations of progress within a sport.
Sports specialization is defined as intensive, year-round training in a single sport at the exclusion of other sports. Early sport specialization may increase rates of overuse injury and sport burnout. Diversified sports training during early and middle adolescence may be more effective in developing elite-level skills in the primary sport due to skill transfer.
High-risk overuse injuries are those that can result in significant loss of time from sport and threaten future participation. Specifically, stress fractures, physeal stress injuries, osteochondritis dissecans, some apophyseal injuries, and effort thrombosis. Due to the immature skeleton, high risk stress fractures include the spine, femoral neck, patella, anterior tibia, medial malleolus, talus, tarsal navicular and metaphyseal/diaphyseal junction of the fifth metatarsal and the sesamoids. Coaches, parents and health care professionals should be highly suspicious of pain reported at these sites. Physeal injuries can occur at the proximal humerus, distal radius, distal femur and the proximal tibia. While physeal stress injuries are self-limiting (resolve with rest), bone growth disturbance and joint deformity may occur. Effort thrombosis in athletes occurs as a consequence of thoracic outlet syndrome. Surgical removal of the first rib often resolves the issue.
Burnout of youth athletes includes the spectrum of overreaching and overtraining. Chronic stress from athletic participation can result in loss of enjoyment, leading to burnout. In children, there appears to be more of a psychological component related to burnout and attrition with adult supervised activities.
Prevention includes limiting weekly and yearly participation time, limits on sport-specific tasks and scheduled rest periods. Modifications should be individualized on the athletes age, growth rate, readiness and injury history. Monitoring of training workload during growth spurts is recommended. Preseason conditioning and neuromuscular training programs can reduce injury rates. Proper sizing of equipment is recommended. To reduce the likelihood of burnout, an emphasis should be placed on skill development more than competition and winning.
In summary, coaches, parents and health care professionals should take an active role in preventing and managing athletes’ training schedules, monitoring their levels of exertion and keep sports participation playful. Youth athletes are particularly susceptible to bone related injuries due to various growth rates and limited resilience of growth plates. Scheduled time off from a single sport, participation in different types of sports, and free-play are all important to foster a larger athletic movement “vocabulary”. While some sports (gymnastics, swimming) benefit from early athletic development, most sports can be specialized on in later adolescence without impeding proficiency.
Physical therapists that specialize in athletes can provide valuable insight for parents and coaches on managing workload, better understanding risk factors for injury, discussing readiness for sports, tradeoffs of sport specialization, education on high-risk overuse injuries and avoiding burnout.
If you are a youth athlete, parent of a youth athlete or coach youth athletics in Miami, Florida and have questions about information presented in this post, give our office a call. We offers seminars to educate the community on best practices for keeping youth athletes participating in sport. As a lifelong athlete myself, I can appreciate the time, effort and role parents and coaches can play in the development of their children. My goal is to keep as many people participating in athletics for as long as possible.