Youth Athlete High Risk Overuse Injuries

Miami's #1 Sports Physical Therapist
Patella stress fractures should be treated with a 4-6 week period of immobilization in a long leg cast. Healing time is typically faster in youth compared to adults. A displaced fracture or nonunion fracture should be referred to an orthopedic surgeon.
Tibial stress fractures have a high risk of nonunion. The “dreaded black line” may be observed on x-rays. If x-rays do not demonstrate a defect, MRI or CT scan may be warranted. Treatment requires a period of non-weightbearing and progressive return to sport. If nonoperative treatment fails, surgical intervention may be necessary.
Ankle stress fractures are uncommon in youth athletes. They are generally treated with rest and gradual return to sport. Stress fractures of the ankle are more common in bounding/jumping sports including gymnastics and dance. If the fracture progresses, surgical intervention may be required.
Tarsal stress fractures are most prevalent in track and field, football and soccer. The most reliable method of identifying this type of fracture is a CT scan. There may be a delay in proper treatment due to the vague nature of complaints from the youth athlete. Poorly fitting footwear may contribute to the development and subsequent aggravation of the fracture.
Parents, coaches, athletes and health care providers should have a high index of suspicion when pain is reported at the site of high risk bone injuries. Localized tenderness over the site, coupled with the athletes history of onset of pain, should warrant imaging by a health care practitioner. Tenderness to touch of the spine and hip may not be reliable, thus, imaging should be done to rule out bony injury.
Radiographs (x-rays) may not be sensitive enough to identify stress reactions/fractures. Further imaging may be necessary (MRI, CT scan) to rule out bone injuries in youth athletes. Treatment of high risk stress reactions and fractures are specific to the site of injury. Very often, a period of rest (non-weightbearing) is required to allow the bone to heal. A progressive and graded return to sport may help prevent subsequent injury.
While there are no studies specific to prevention of stress fractures in youth athletes, the general consensus is similar to adults. Limiting high impact activities, optimizing vitamin D and calcium intake, screening for the female athlete triad and proper footwear should be assessed. Early recognition is key to optimal treatment.
If you are a youth athlete, parent of a youth athlete or coach youth athletics in Miami, Florida and have questions about information presented in this post, give our office a call. We offers seminars to educate the community on best practices for keeping youth athletes participating in sport. As a lifelong athlete myself, I can appreciate the time, effort and role parents and coaches can play in the development of their children. My goal is to keep as many people participating in athletics for as long as possible.
While stress fractures of the femoral neck are not common in children and adolescents, if not recognized early and treated, complete fracture may occur. If an athlete is complaining of hip or groin pain in the front, the health care provider, coach and parent should be highly suspicious. Depending on the location of the fracture, referral to an orthopedic surgeon is necessary. A period of non-weightbearing may be required to allow the bone to heal.
Patella stress fractures should be treated with a 4-6 week period of immobilization in a long leg cast. Healing time is typically faster in youth compared to adults. A displaced fracture or nonunion fracture should be referred to an orthopedic surgeon.
Tibial stress fractures have a high risk of nonunion. The “dreaded black line” may be observed on x-rays. If x-rays do not demonstrate a defect, MRI or CT scan may be warranted. Treatment requires a period of non-weightbearing and progressive return to sport. If nonoperative treatment fails, surgical intervention may be necessary.
Ankle stress fractures are uncommon in youth athletes. They are generally treated with rest and gradual return to sport. Stress fractures of the ankle are more common in bounding/jumping sports including gymnastics and dance. If the fracture progresses, surgical intervention may be required.
Tarsal stress fractures are most prevalent in track and field, football and soccer. The most reliable method of identifying this type of fracture is a CT scan. There may be a delay in proper treatment due to the vague nature of complaints from the youth athlete. Poorly fitting footwear may contribute to the development and subsequent aggravation of the fracture.
Parents, coaches, athletes and health care providers should have a high index of suspicion when pain is reported at the site of high risk bone injuries. Localized tenderness over the site, coupled with the athletes history of onset of pain, should warrant imaging by a health care practitioner. Tenderness to touch of the spine and hip may not be reliable, thus, imaging should be done to rule out bony injury.
Radiographs (x-rays) may not be sensitive enough to identify stress reactions/fractures. Further imaging may be necessary (MRI, CT scan) to rule out bone injuries in youth athletes. Treatment of high risk stress reactions and fractures are specific to the site of injury. Very often, a period of rest (non-weightbearing) is required to allow the bone to heal. A progressive and graded return to sport may help prevent subsequent injury.
While there are no studies specific to prevention of stress fractures in youth athletes, the general consensus is similar to adults. Limiting high impact activities, optimizing vitamin D and calcium intake, screening for the female athlete triad and proper footwear should be assessed. Early recognition is key to optimal treatment.
If you are a youth athlete, parent of a youth athlete or coach youth athletics in Miami, Florida and have questions about information presented in this post, give our office a call. We offers seminars to educate the community on best practices for keeping youth athletes participating in sport. As a lifelong athlete myself, I can appreciate the time, effort and role parents and coaches can play in the development of their children. My goal is to keep as many people participating in athletics for as long as possible.
About half of youth athletes evaluated for low back pain presented with occult spondylosis. Nonunion of the bone ranged between 14-70%, with those being untreated being more likely to experience nonunion. On average, about 5.4 months off from sport was required for bone healing. This typically included bracing, but an individual approach best determines which intervention is necessary. Surgical pars repair (fusion) may be necessary if no union is demonstrated at 6 months.
While stress fractures of the femoral neck are not common in children and adolescents, if not recognized early and treated, complete fracture may occur. If an athlete is complaining of hip or groin pain in the front, the health care provider, coach and parent should be highly suspicious. Depending on the location of the fracture, referral to an orthopedic surgeon is necessary. A period of non-weightbearing may be required to allow the bone to heal.
Patella stress fractures should be treated with a 4-6 week period of immobilization in a long leg cast. Healing time is typically faster in youth compared to adults. A displaced fracture or nonunion fracture should be referred to an orthopedic surgeon.
Tibial stress fractures have a high risk of nonunion. The “dreaded black line” may be observed on x-rays. If x-rays do not demonstrate a defect, MRI or CT scan may be warranted. Treatment requires a period of non-weightbearing and progressive return to sport. If nonoperative treatment fails, surgical intervention may be necessary.
Ankle stress fractures are uncommon in youth athletes. They are generally treated with rest and gradual return to sport. Stress fractures of the ankle are more common in bounding/jumping sports including gymnastics and dance. If the fracture progresses, surgical intervention may be required.
Tarsal stress fractures are most prevalent in track and field, football and soccer. The most reliable method of identifying this type of fracture is a CT scan. There may be a delay in proper treatment due to the vague nature of complaints from the youth athlete. Poorly fitting footwear may contribute to the development and subsequent aggravation of the fracture.
Parents, coaches, athletes and health care providers should have a high index of suspicion when pain is reported at the site of high risk bone injuries. Localized tenderness over the site, coupled with the athletes history of onset of pain, should warrant imaging by a health care practitioner. Tenderness to touch of the spine and hip may not be reliable, thus, imaging should be done to rule out bony injury.
Radiographs (x-rays) may not be sensitive enough to identify stress reactions/fractures. Further imaging may be necessary (MRI, CT scan) to rule out bone injuries in youth athletes. Treatment of high risk stress reactions and fractures are specific to the site of injury. Very often, a period of rest (non-weightbearing) is required to allow the bone to heal. A progressive and graded return to sport may help prevent subsequent injury.
While there are no studies specific to prevention of stress fractures in youth athletes, the general consensus is similar to adults. Limiting high impact activities, optimizing vitamin D and calcium intake, screening for the female athlete triad and proper footwear should be assessed. Early recognition is key to optimal treatment.
If you are a youth athlete, parent of a youth athlete or coach youth athletics in Miami, Florida and have questions about information presented in this post, give our office a call. We offers seminars to educate the community on best practices for keeping youth athletes participating in sport. As a lifelong athlete myself, I can appreciate the time, effort and role parents and coaches can play in the development of their children. My goal is to keep as many people participating in athletics for as long as possible.
While most stress fractures heal with appropriate rest, rehabilitation and progressive return to sport, certain stress reactions or fractures do not heal readily. These are deemed “high risk”. Improper identification and treatment can lead to nonunion, chronic pain or lead to degenerative joint disease. Delayed union has been reported to occur in up to 10% of athletic stress fractures.
About half of youth athletes evaluated for low back pain presented with occult spondylosis. Nonunion of the bone ranged between 14-70%, with those being untreated being more likely to experience nonunion. On average, about 5.4 months off from sport was required for bone healing. This typically included bracing, but an individual approach best determines which intervention is necessary. Surgical pars repair (fusion) may be necessary if no union is demonstrated at 6 months.
While stress fractures of the femoral neck are not common in children and adolescents, if not recognized early and treated, complete fracture may occur. If an athlete is complaining of hip or groin pain in the front, the health care provider, coach and parent should be highly suspicious. Depending on the location of the fracture, referral to an orthopedic surgeon is necessary. A period of non-weightbearing may be required to allow the bone to heal.
Patella stress fractures should be treated with a 4-6 week period of immobilization in a long leg cast. Healing time is typically faster in youth compared to adults. A displaced fracture or nonunion fracture should be referred to an orthopedic surgeon.
Tibial stress fractures have a high risk of nonunion. The “dreaded black line” may be observed on x-rays. If x-rays do not demonstrate a defect, MRI or CT scan may be warranted. Treatment requires a period of non-weightbearing and progressive return to sport. If nonoperative treatment fails, surgical intervention may be necessary.
Ankle stress fractures are uncommon in youth athletes. They are generally treated with rest and gradual return to sport. Stress fractures of the ankle are more common in bounding/jumping sports including gymnastics and dance. If the fracture progresses, surgical intervention may be required.
Tarsal stress fractures are most prevalent in track and field, football and soccer. The most reliable method of identifying this type of fracture is a CT scan. There may be a delay in proper treatment due to the vague nature of complaints from the youth athlete. Poorly fitting footwear may contribute to the development and subsequent aggravation of the fracture.
Parents, coaches, athletes and health care providers should have a high index of suspicion when pain is reported at the site of high risk bone injuries. Localized tenderness over the site, coupled with the athletes history of onset of pain, should warrant imaging by a health care practitioner. Tenderness to touch of the spine and hip may not be reliable, thus, imaging should be done to rule out bony injury.
Radiographs (x-rays) may not be sensitive enough to identify stress reactions/fractures. Further imaging may be necessary (MRI, CT scan) to rule out bone injuries in youth athletes. Treatment of high risk stress reactions and fractures are specific to the site of injury. Very often, a period of rest (non-weightbearing) is required to allow the bone to heal. A progressive and graded return to sport may help prevent subsequent injury.
While there are no studies specific to prevention of stress fractures in youth athletes, the general consensus is similar to adults. Limiting high impact activities, optimizing vitamin D and calcium intake, screening for the female athlete triad and proper footwear should be assessed. Early recognition is key to optimal treatment.
If you are a youth athlete, parent of a youth athlete or coach youth athletics in Miami, Florida and have questions about information presented in this post, give our office a call. We offers seminars to educate the community on best practices for keeping youth athletes participating in sport. As a lifelong athlete myself, I can appreciate the time, effort and role parents and coaches can play in the development of their children. My goal is to keep as many people participating in athletics for as long as possible.
High risk overuse injuries in youth athletes may be exacerbated if they are unrecognized or inappropriately treated. This can lead to significant time off from sport and threaten future participation. High risk injuries include stress fractures, physeal stress injuries, osteochondritis dessicans, some apophyseal injuries and effort thrombosis.
Let’s take a look at these in further detail.
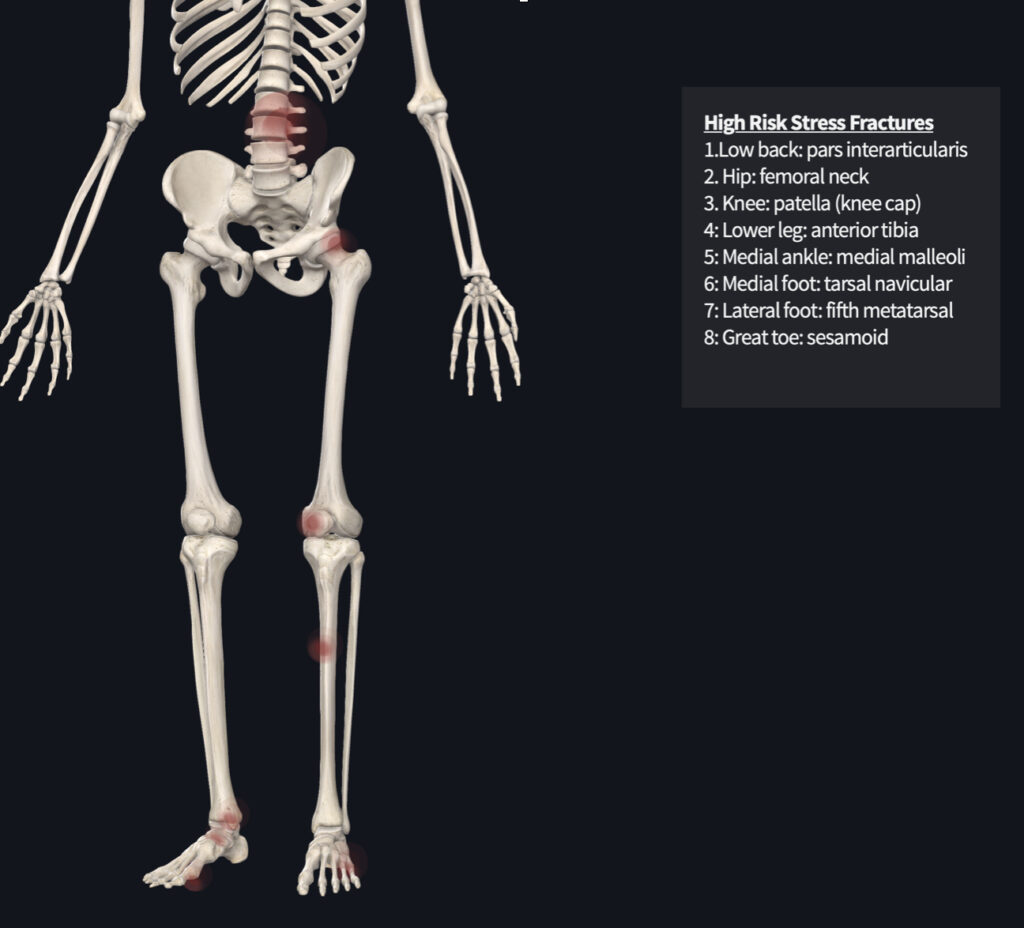
While most stress fractures heal with appropriate rest, rehabilitation and progressive return to sport, certain stress reactions or fractures do not heal readily. These are deemed “high risk”. Improper identification and treatment can lead to nonunion, chronic pain or lead to degenerative joint disease. Delayed union has been reported to occur in up to 10% of athletic stress fractures.
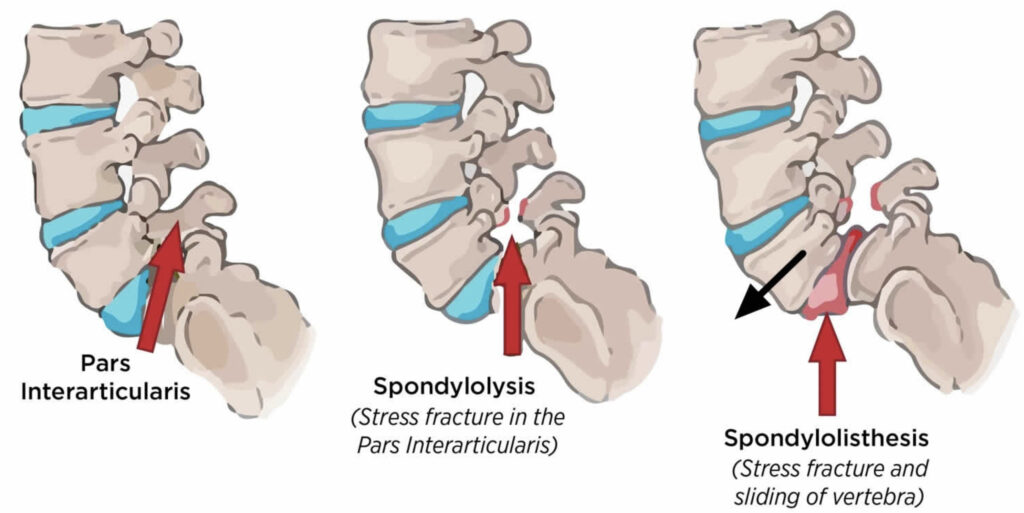
About half of youth athletes evaluated for low back pain presented with occult spondylosis. Nonunion of the bone ranged between 14-70%, with those being untreated being more likely to experience nonunion. On average, about 5.4 months off from sport was required for bone healing. This typically included bracing, but an individual approach best determines which intervention is necessary. Surgical pars repair (fusion) may be necessary if no union is demonstrated at 6 months.
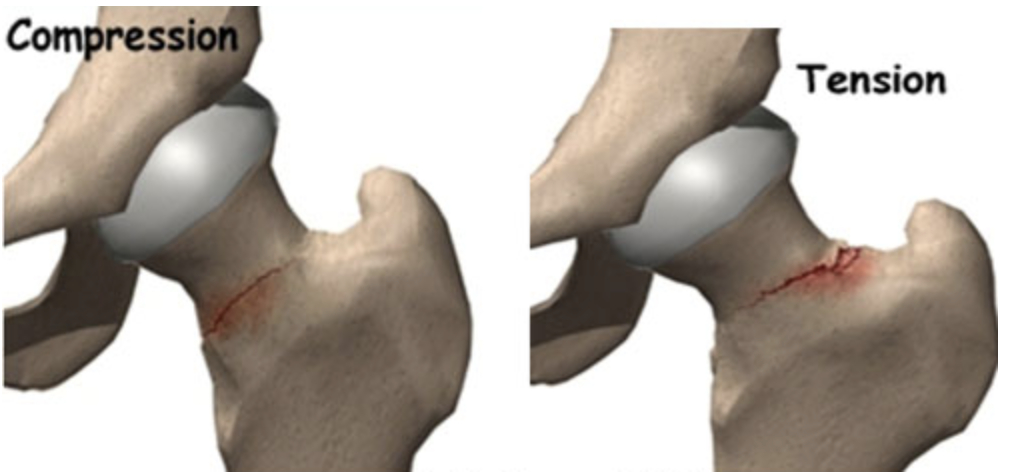
While stress fractures of the femoral neck are not common in children and adolescents, if not recognized early and treated, complete fracture may occur. If an athlete is complaining of hip or groin pain in the front, the health care provider, coach and parent should be highly suspicious. Depending on the location of the fracture, referral to an orthopedic surgeon is necessary. A period of non-weightbearing may be required to allow the bone to heal.
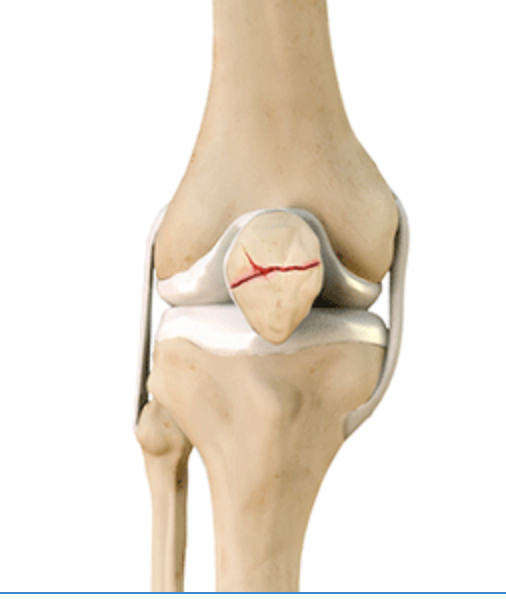
Patella stress fractures should be treated with a 4-6 week period of immobilization in a long leg cast. Healing time is typically faster in youth compared to adults. A displaced fracture or nonunion fracture should be referred to an orthopedic surgeon.
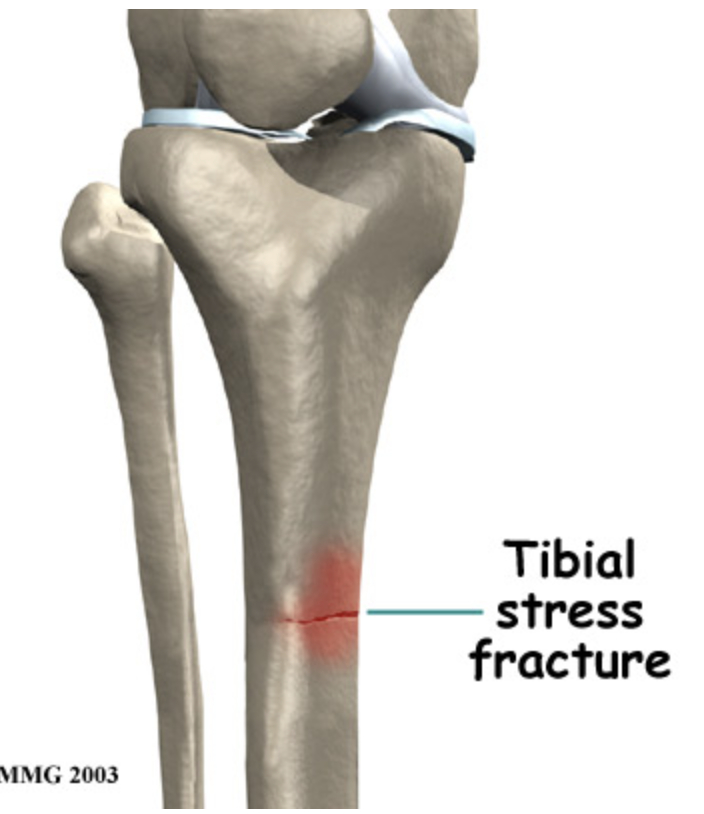
Tibial stress fractures have a high risk of nonunion. The “dreaded black line” may be observed on x-rays. If x-rays do not demonstrate a defect, MRI or CT scan may be warranted. Treatment requires a period of non-weightbearing and progressive return to sport. If nonoperative treatment fails, surgical intervention may be necessary.
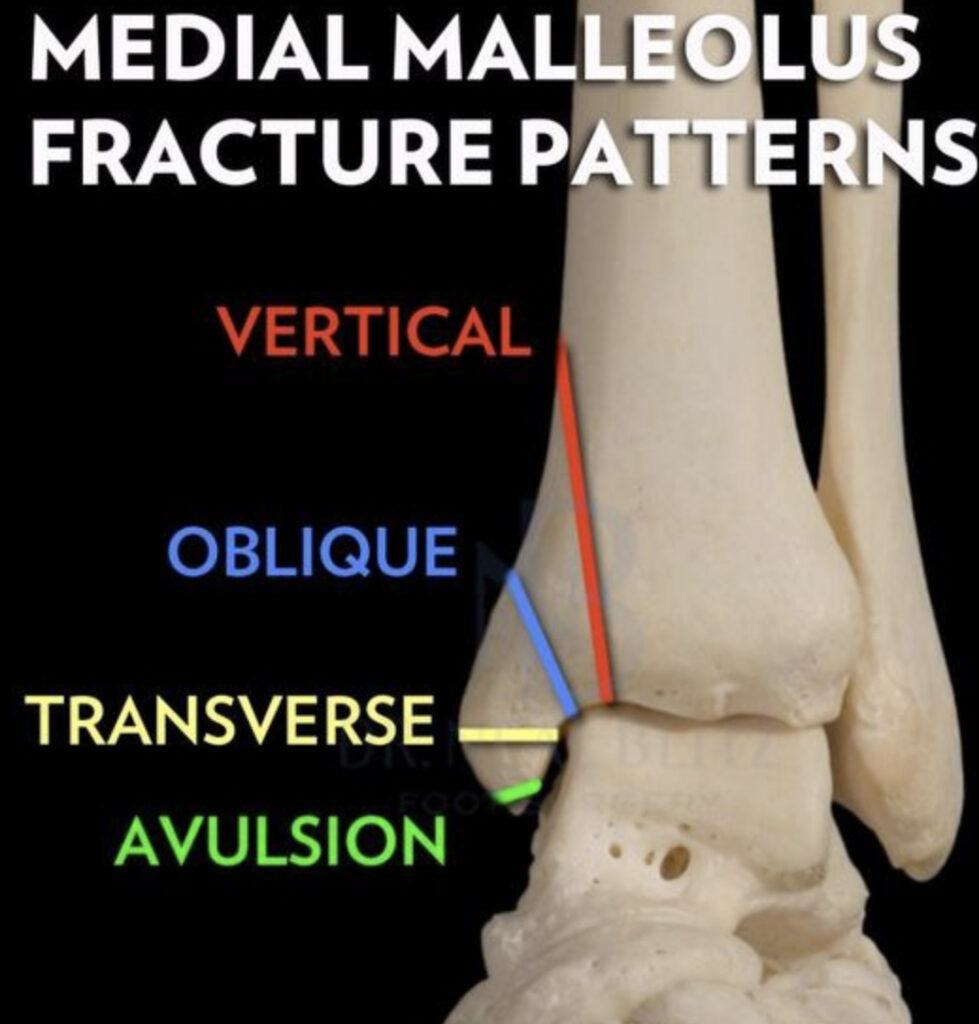
Ankle stress fractures are uncommon in youth athletes. They are generally treated with rest and gradual return to sport. Stress fractures of the ankle are more common in bounding/jumping sports including gymnastics and dance. If the fracture progresses, surgical intervention may be required.
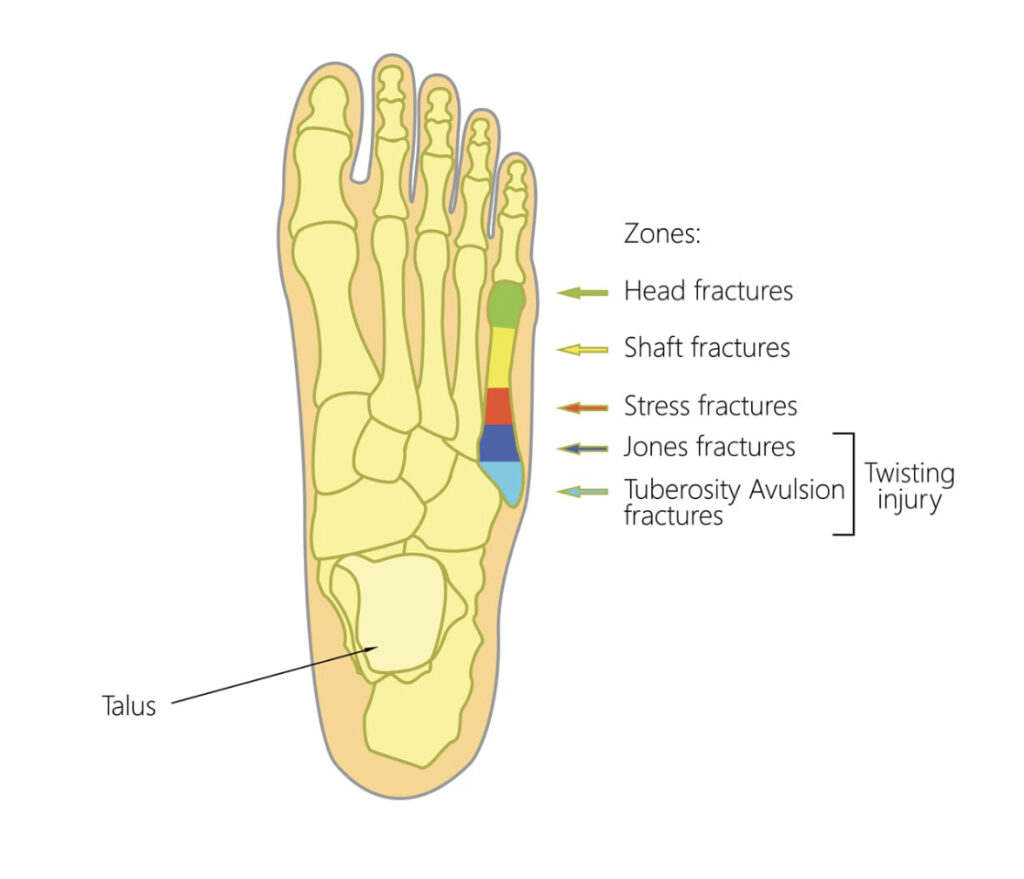
Tarsal stress fractures are most prevalent in track and field, football and soccer. The most reliable method of identifying this type of fracture is a CT scan. There may be a delay in proper treatment due to the vague nature of complaints from the youth athlete. Poorly fitting footwear may contribute to the development and subsequent aggravation of the fracture.
Parents, coaches, athletes and health care providers should have a high index of suspicion when pain is reported at the site of high risk bone injuries. Localized tenderness over the site, coupled with the athletes history of onset of pain, should warrant imaging by a health care practitioner. Tenderness to touch of the spine and hip may not be reliable, thus, imaging should be done to rule out bony injury.
Radiographs (x-rays) may not be sensitive enough to identify stress reactions/fractures. Further imaging may be necessary (MRI, CT scan) to rule out bone injuries in youth athletes. Treatment of high risk stress reactions and fractures are specific to the site of injury. Very often, a period of rest (non-weightbearing) is required to allow the bone to heal. A progressive and graded return to sport may help prevent subsequent injury.
While there are no studies specific to prevention of stress fractures in youth athletes, the general consensus is similar to adults. Limiting high impact activities, optimizing vitamin D and calcium intake, screening for the female athlete triad and proper footwear should be assessed. Early recognition is key to optimal treatment.
If you are a youth athlete, parent of a youth athlete or coach youth athletics in Miami, Florida and have questions about information presented in this post, give our office a call. We offers seminars to educate the community on best practices for keeping youth athletes participating in sport. As a lifelong athlete myself, I can appreciate the time, effort and role parents and coaches can play in the development of their children. My goal is to keep as many people participating in athletics for as long as possible.

The physis is the part of the bone where the growth plates are located. These structures are relatively weak compared to the surrounding bone because the cells have not yet matured. Excessive compression or shearing (sliding) that occurs at these regions expose the bone to injury.
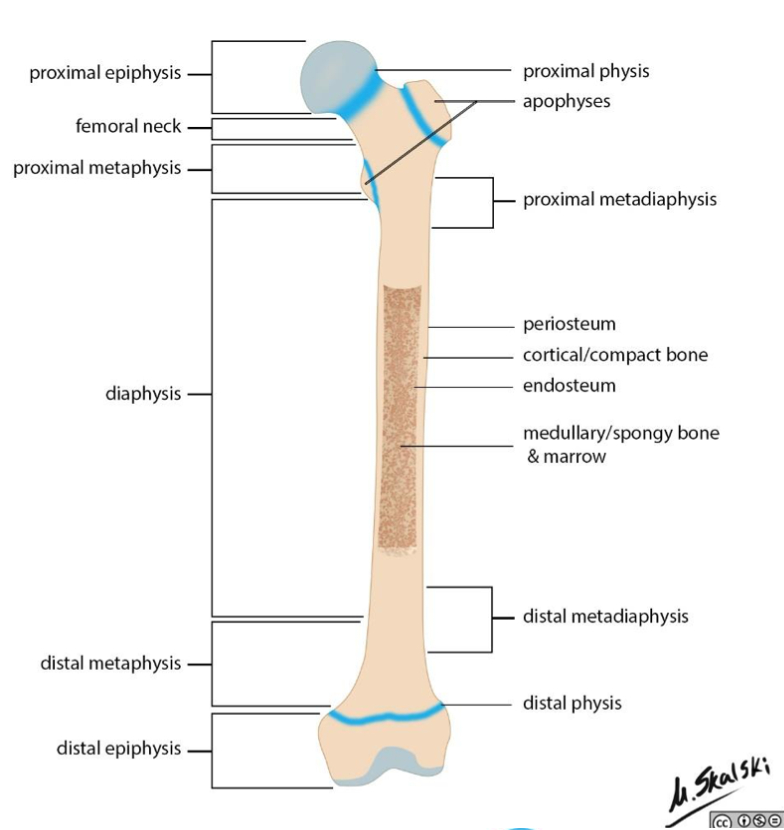
Stress injury to the physis may permanently deform the bone, leading to bone length discrepancy malalignment of the affected limb. In adolescent athletes, the proximal humerus (shoulder), distal radius (wrist), distal femur (knee) and proximal tibia (knee) are most prone to injury. High stress activities like gymnastics and field sports have high incidence rates due to high impact movements. Between 10-85% of gymnasts demonstrate radiographic evidence of physeal stress reactions.
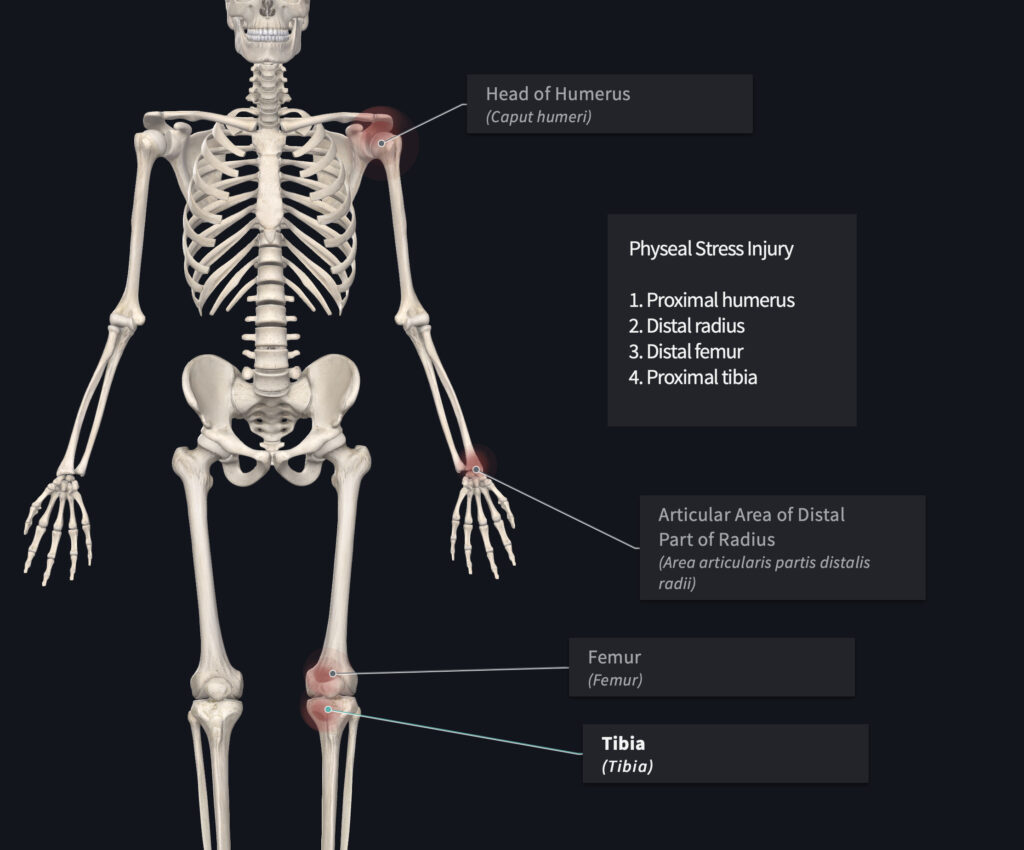
Secondary pathology may occur including impingement of soft tissue (TFCC in the wrist), degenerative joint disease, and chronic pain. Involvement of the knee may lead to the development of bow-legged (genu varum) pathology.
Physeal stress injuries are often treated with rest and limited weight bearing on the affected limb. Allowing time for the growth plate to properly develop can mitigate the effects of altered limb length discrepancy and joint deformity.
If you are a youth athlete, parent of a youth athlete or coach youth athletics in Miami, Florida and have questions about information presented in this post, give our office a call. We offers seminars to educate the community on best practices for keeping youth athletes participating in sport. As a lifelong athlete myself, I can appreciate the time, effort and role parents and coaches can play in the development of their children. My goal is to keep as many people participating in athletics for as long as possible.

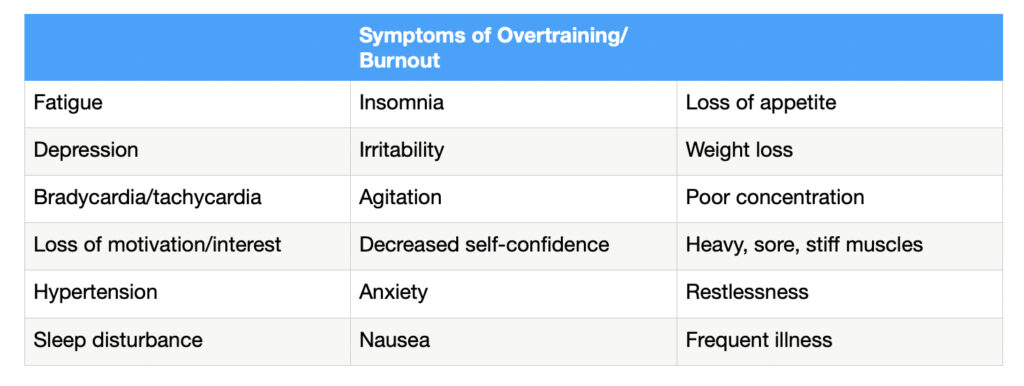
Burnout in youth athletics is part of a spectrum of conditions that includes overreaching and overtraining. It is defined to occur when chronic stress causes the youth athlete to cease participation in sport. Sports specialization may play a role as youth athletes may withdraw from sport either due to injury or burnout. In children, the psychological component related to burnout and attrition may be related to adult supervised activities.
Overreaching can be classified as either functional or non-functional. Nonfuncitonal overreaching is defined as intense training that leads to a longer period of decreased performance. It may be accompanied by increased psychological or neuroendocronological symptoms. These include physiological and hormonal changes that result in decreased sports performance.
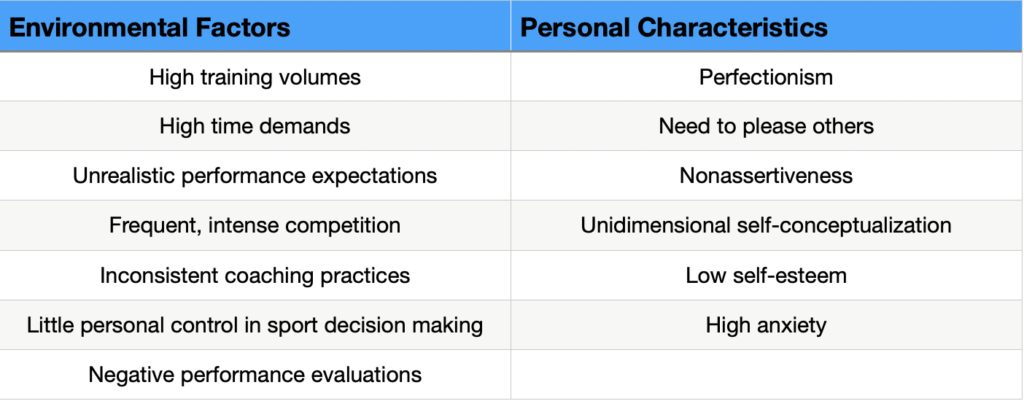
While no specific test or questionnaire currently exists to identify burnout, certain characteristics of sports participation may predispose youth athletes to burnout. These include full participation in a single sport, without participation in unsupervised activities.
Four states of burnout can be described as 1) the young athlete is placed in a situation that involves varying demands; 2) the demands are perceived as excessive; 3) the young athlete experiences varying physiological responses; and 4) varying burnout consequences (withdrawal from sport).
Sports participation that includes a “fun play” may ameliorate anxiety, low self esteem and low personal performance. Excessive athletic stress can lead to loss of sleep, poor appetite, decreased satisfaction with sport, physical injury, low performance and eventual withdrawal. While stress (eustress) is a necessary component of growth (character & sports development), it needs to be appropriately managed.
If your youth athlete is experiencing depression, anxiety and sleep disturbances, consulting a mental health expert (sports psychologist) may help address the underlying issue. While parents may feel vulnerable discussing mental health issues due to social stigma, it is important to understand that mental health experts are properly positioned to get treat psychological disturbances. Think of it like this- if your child broke their arm, you wouldn’t hesitate to take them to the hospital. Speaking with a mental health counselor should be no different. In fact, it is my opinion that positive psychology can have a profound impact of an athletes performance. But that is best discussed with a professional in their field.
From a physical therapists perspective, the workload of an athlete can be monitored, as well as an athletes perception of “play”- keeping it light yet competitive.

The medical literature has proposed several factors that may contribute to overuse injuries. These are often grouped into intrinsic and extrinsic factors. Intrinsic factors include variations in growth and development, anatomic alignment, muscle-tendon imbalance, flexibility, conditioning, biomechanics, and history of prior injury. Extrinsic factors include workload, sport technique, training environment, and equipment. Each athlete is unique in their attributes, each sport is unique in their specific risk factors.
The complex interaction between intrinsic (individual) and extrinsic (environment) creates a challenge to injury prevention and treatment. Some risk factors are modifiable- including strength, aerobic conditioning and workload. Other risk factors are non-modifiable- gender, age, injury history. Recognizing the relationship between risk factors can help develop injury prevention strategies.
We will take a further look at the following intrinsic risk factors for athletes: previous injury history; growth and development; anatomic alignment; flexibility; biomechanics; strength and conditioning; and menstrual irregularity.

Extrinsic risk factors are largely modifiable. These include sport technique and biomechanics, volume and intensity of workloads, scheduling, training environment and equipment.
Weak causal evidence is available regarding risk factors for overuse injuries in youth athletes, therefore, more research is needed to help clinicians better understand these mechanisms. Each sport presents with unique movement patterns and each athlete presents with unique character traits. This adds to the complexity of conducting research and developing appropriate guidelines for physical therapists, coaches and athletes to follow.
If you are a youth athlete, parent of a youth athlete or coach youth athletics in Miami, Florida and have questions about information presented in this post, give our office a call. We offers seminars to educate the community on best practices for keeping youth athletes participating in sport. As a lifelong athlete myself, I can appreciate the time, effort and role parents and coaches can play in the development of their children. My goal is to keep as many people participating in athletics for as long as possible.

Overuse injuries in youth athletes is a complex interaction of multiple factors. Unique to this population are growth-related factors, which present a challenge to injury prevention and rehabilitation. While youth sports related injuries can be self-limited, they can also be lengthy and may result in lifelong impairments. It is important that health care providers offer a comprehensive evaluation and treatment to prevent burnout and mitigate permanent deformity.
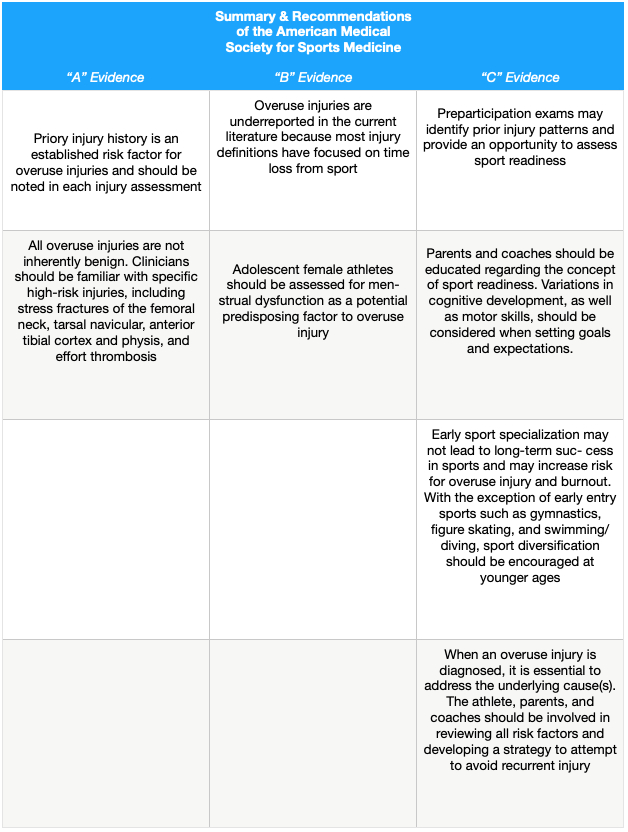
Below is a chart that summarizes the current recommendations. They are categorized into the strength of each domain, with “A” having strong support, “B” moderate support and “C” limited support from the literature. This is not to say that “B” or “C” level evidence is not useful, only that the recommendation is based on limited research. The recommendations are based on the American Medical Society for Sports Medicine, and compiled in 2014.

While studies have failed to demonstrate successful overuse injury methods, current recommendations follow rather loose guidelines that may help parents, coaches and physical therapists. These recommendations are based on the current available information. These include training workload, strength training, equipment and burnout.
Relatively high workloads for youth athletes may increase the risk of overuse injuries. Suggestions based on current literature include limiting weekly and yearly participation times for sport-specific movements. Pitching count limits, for example, may result in elbow pain in baseball pitchers. Monitoring of training workload during growth spurts is advised due to the asynchronous growth of body parts.

Strength training including preseason resistance and cardiovascular conditioning may help prepare an athlete for sport-specific demands. Neuromuscular training (balance and coordination) may help reduce lower extremity injuries in field sports. Contrary to popular belief, regular participation in resistance training is beneficial to, and can reduce injury rates in youth athletes. These include improved bone density, more resilient ligaments and stronger muscles.
Frequent evaluation of equipment during growth spurts should be implemented. Although the research does not demonstrate a correlation between overuse and poor fitting equipment, a hypothetical alteration in biomechanics may occur. If the coach, parent or athlete is experiencing problems with ill-fitting equipment, it should be addressed in a timely fashion.
Avoidance of over scheduling and excessive time commitment to sport may prevent burnout. For youth athletes, emphasis should be placed on skill development over competition and winning.
If you are a youth athlete, parent of a youth athlete or coach youth athletics in Miami, Florida and have questions about information presented in this post, give our office a call. We offers seminars to educate the community on best practices for keeping youth athletes participating in sport. As a lifelong athlete myself, I can appreciate the time, effort and role parents and coaches can play in the development of their children. My goal is to keep as many people participating in athletics for as long as possible.

Enjoy this video about how physical therapy can help athletes return to sport after injury.
Current research shows that a structured and progressive return to sport after injury can help reduce subsequent injury and improve performance, helping you get back on to competition schedule and gaining confidence.
We can help coaches, parents and athletes better understand the demands of sport and minimize the guesswork of how to get back to training and competing safely.
The research in this field is ongoing as sport specific demands, individual attributes including injury history and previous training schedule, as well as competition schedule can influence the specific program you need to get back on track.
If you are an athlete in Miami, FL recovering from an injury and need some guidance on how to best return to your sport, give us a call and we can help you out!
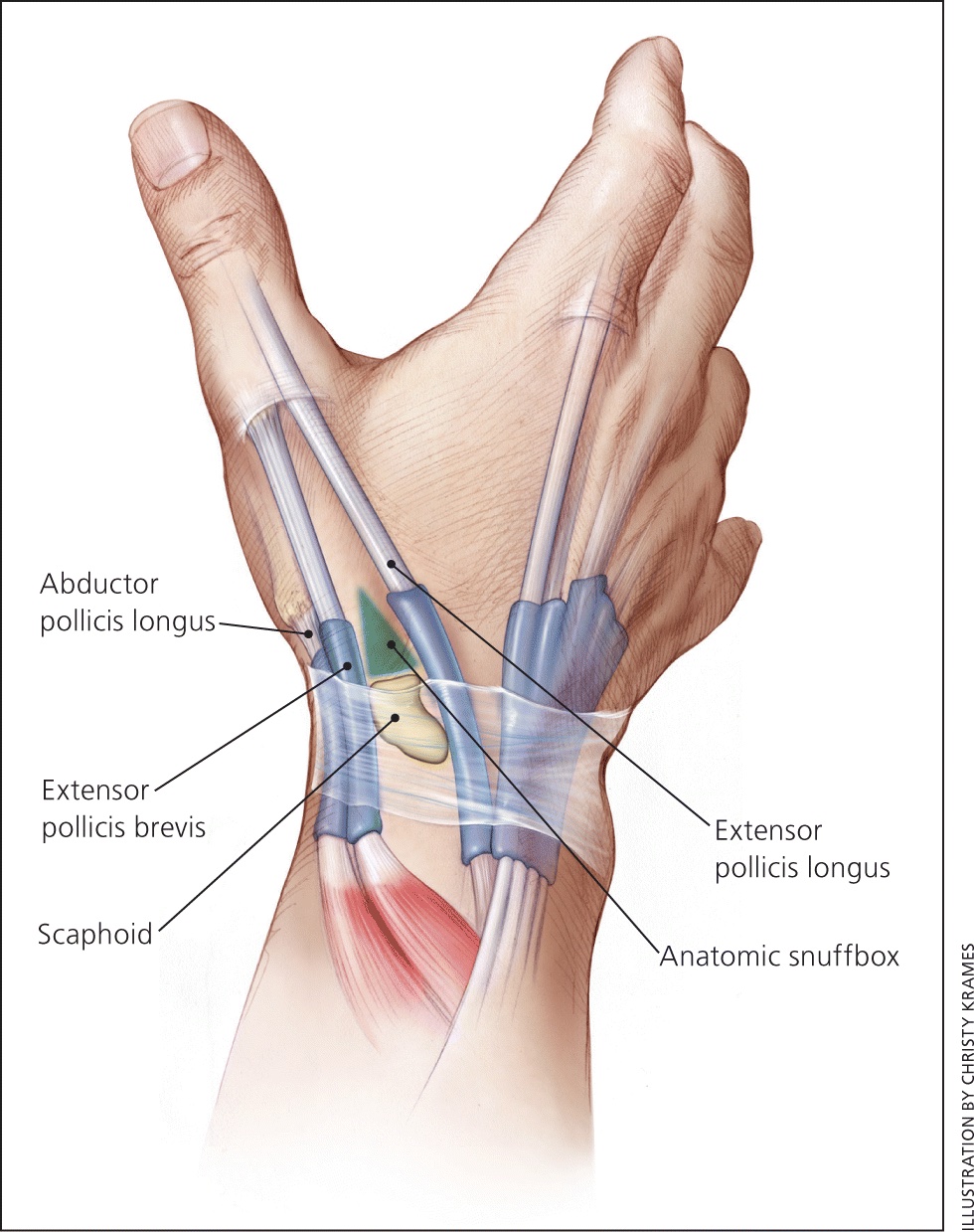
In this video we will be discussing a common cause of wrist pain and dysfunction in athletes: scapholunate instability.
Lets review some anatomy first.
The wrist joint is formed by the scaphoid and lunate bones forming a “keystone” of the arch of the wrist, connecting with the radius bone of the forearm.
The stability of the scaphoid and lunate is formed primarily by the scapholunate interosseous ligament and secondarily by several additional layers on the palm and back of the hand.
The scapholunate interosseous ligament may be disrupted- either by a single traumatic incident like a fall on an outstretched hand, or by repetitive micro trauma, like back handsprings in gymnasts, or when pressure is applied to the body when a grappler is performing a technical standup.
This creates a mechanical change in how the wrist functions. The stress that would normally be directed through this “keystone”, is shifted to other structures of the wrist, often causing pain, instability or limiting range of motion. Athletes may also report weakness with gripping activities.
The secondary support structures of the wrist may become overstressed and the athlete may experience subsequent trauma. This may include joint degeneration, ligamentous instability, and in rare cases, avascular necrosis of the scaphoid bone.
While surgical intervention is not usually needed, conservative care is often the first line of treatment to reduce pain, restore wrist mobility and improve strength with sports related tasks.
Athletes performing the following tasks may experience this type of wrist pain: the front rack position (weightlifting, crossfit), backhand springs (gymnastics), punching (boxers, MMA), technical stand up (grapplers, wrestlers, brazilian jiu jitsu).
If you are an athlete in Miami experiencing wrist pain with sports participation, give our office a call. We can help you manage this issue without medicine, injections or surgery.

In this video we will be discussing a common cause of elbow pain and dysfunction in grappling athletes after getting arm barred.
The elbow joint is formed by three bones: the humerus, ulna and radius.
The joint is reinforced by ligaments wrapping around the head of the radius and humerus; and between the ulna and humerus.
The bicep and brachialis flex (bends) the elbow. They are the primary muscles when resisting the arm bar by flexing the elbow.
When the elbow is brought to full extension, when the grappler is tapping, the “hook” of the ulna comes into contact with the “pit” on the back of the humerus.
The surface of the joint is soft and spongy, and very sensitive to stress. The surface of the joint is aggressively compressed, causing damage.
Repetitive injury to the joint surface can cause in early onset joint degeneration (arthritis), leading to loss of range of motion, muscular weakness and pain.
In some cases, a fragment may dislodge from the joint surface and float around within the joint. This may cause clicking, catching or locking. Over time, this fragment may become larger, causing further damage. If the athlete is experiencing significant dysfunction, surgical intervention may be required.
The ulnar collateral ligament can also be involved. Injury to the ligament can lead to joint instability, causing further damage to the joint, and possible nerve entrapment.
With most cases, physical therapy can help restore joint mobility, improve muscle strength, manage pain and facilitate a return to sport.
If you are a grappler (wrestling, judo, jiu jitsu, mma) and experiencing elbow pain, give our office a call. We can help you manage this injury without the use of surgery, injections or medicine.

This video describes relevant hand and wrist anatomy. It is a brief overview of how the hand functions in relation to sports related tasks.